

Abstract
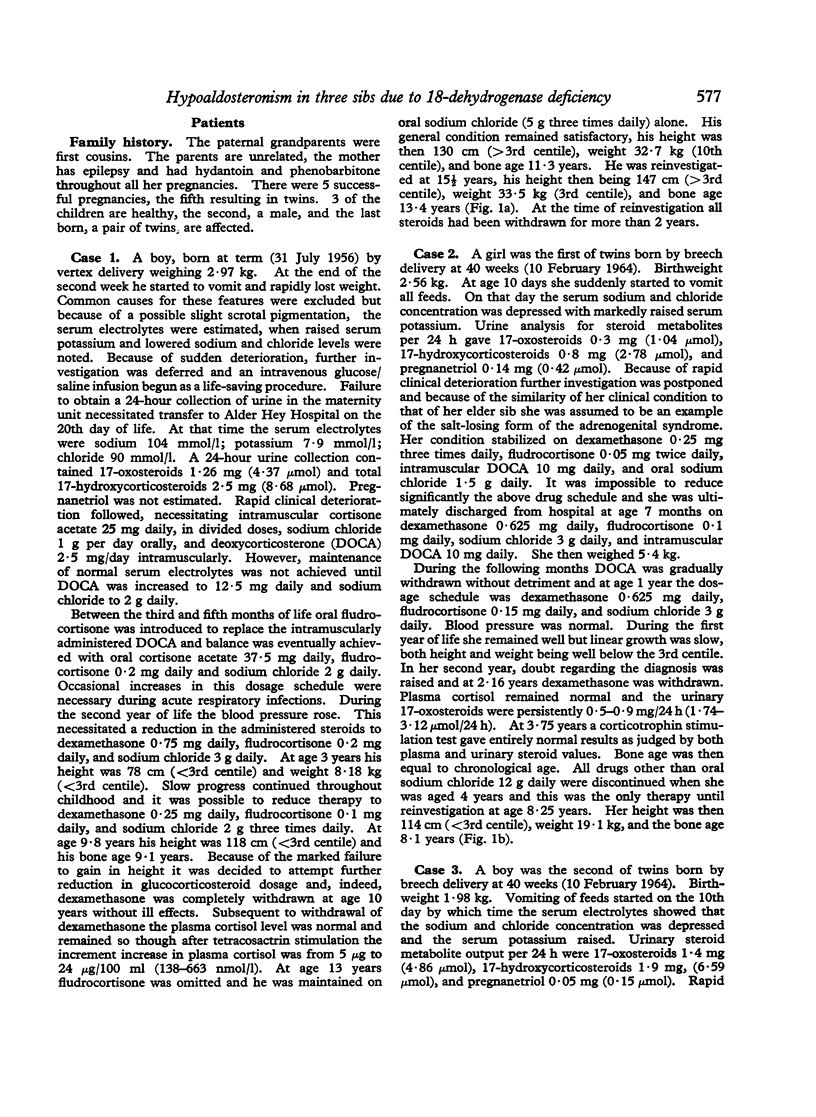
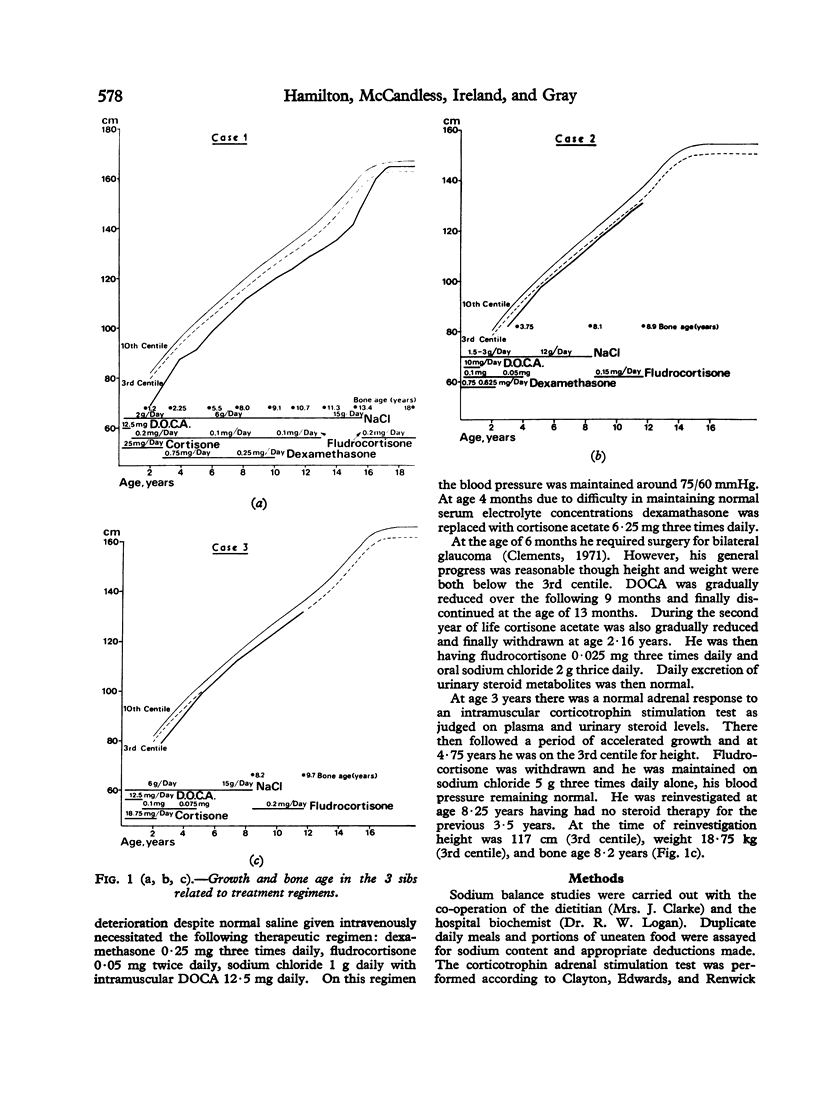
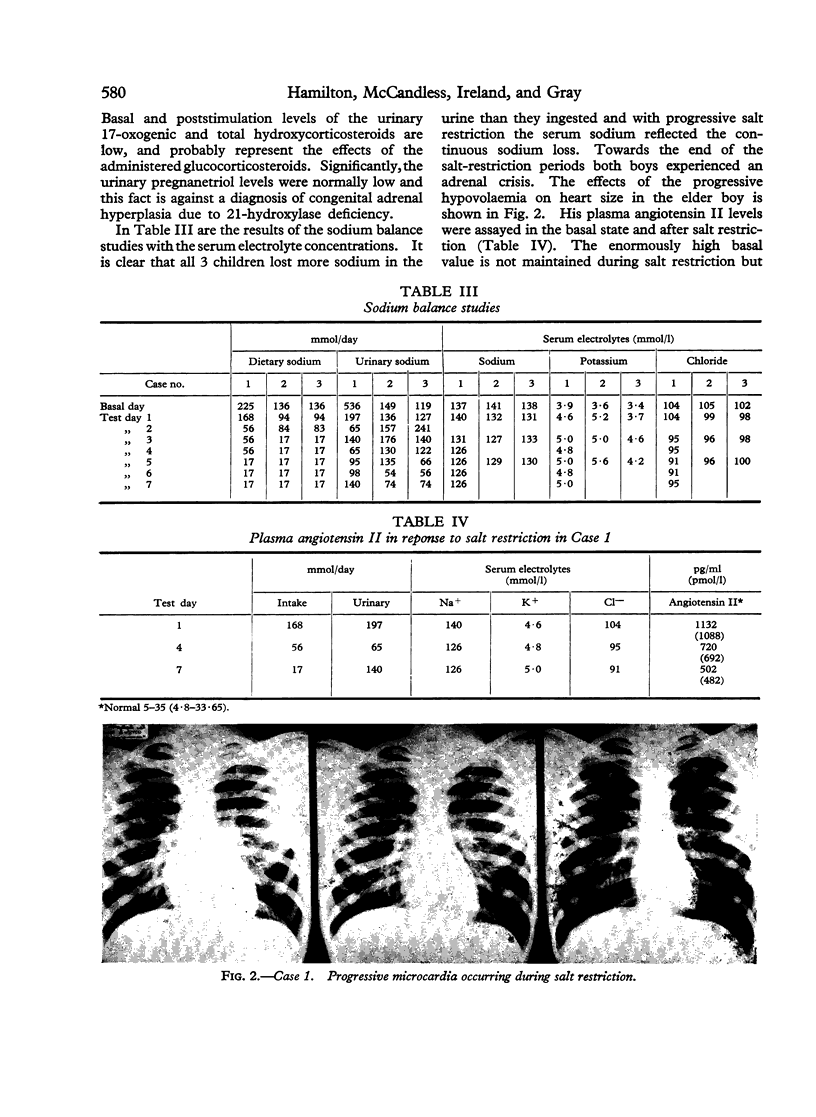
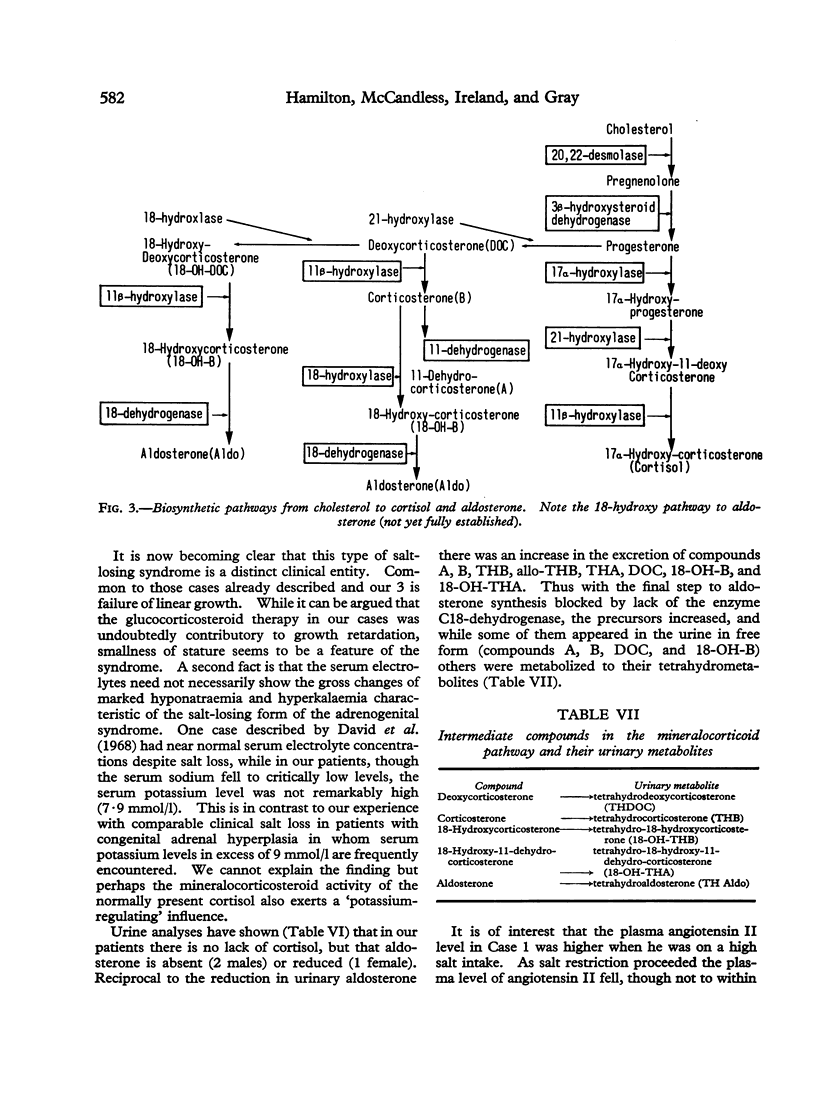
Three sibs all presented in the early neonatal period with a salt-losing syndrome. The salt-losing form of congenital adrenal hyperplasia was diagnosed and appropriate treatment with glucocorticosteroids, mineralocorticosteroids, and additional dietary salt started. Although early life was maintained with difficulty, with age all 3 children required decreasing amounts of replacement steroids to maintain normal plasma electrolyte balance. They were reinvestigated at the ages of 15 years and 8 years (twins), when cortisol synthesis and metabolism proved normal, but aldosterone synthesis was blocked by deficiency of 18-dehydrogenase. Rational treatment of these cases of a salt-losing syndrome in which aldosterone synthesis alone is blocked due to lack of the enzyme 18-dehydrogenase requires the administration of a mineralocorticosteroid drug only. Since deoxycorticosterone (acetate or pivalate) requires intramuscular administration, as life-long therapy oral fludrocortisone is preferable. Although fludrocortisone has glucocorticoid activity, the "hydrocortisone equivalent" effect of the small dosage used was unlikely to inhibit either pituitary corticotrophin or growth hormone production.
Full text
PDF

Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- CLAYTON B. E., EDWARDS R. W., RENWICK A. G. Adrenal function in children. Arch Dis Child. 1963 Feb;38:49–53. doi: 10.1136/adc.38.197.49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clements D. B. Adrenogenital syndrome and buphthalmos. Br J Ophthalmol. 1971 Apr;55(4):275–278. doi: 10.1136/bjo.55.4.275. [DOI] [PMC free article] [PubMed] [Google Scholar]
- David R., Golan S., Drucker W. Familial aldosterone deficiency: enzyme defect, diagnosis, and clinical course. Pediatrics. 1968 Feb;41(2):403–412. [PubMed] [Google Scholar]
- Gardiner W. L., Herning E. C. Gas-liquid chromatographic separation of C19 and C21 human urinary steroids by a new procedure. Biochim Biophys Acta. 1966 Feb 28;115(2):524–526. doi: 10.1016/0304-4165(66)90461-2. [DOI] [PubMed] [Google Scholar]
- RUSSELL A., LEVIN B., SINCLAIR L., OBERHOLZER V. G. A REVERSIBLE SALT-WASTING SYNDROME OF THE NEWBORN AND INFANT: POSSIBLE INFANTILE HYPOALDOSTERONISM. Arch Dis Child. 1963 Aug;38:313–325. doi: 10.1136/adc.38.200.313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- ULICK S., GAUTIER E., VETTER K. K., MARKELLO J. R., YAFFE S., LOWE C. U. AN ALDOSTERONE BIOSYNTHETIC DEFECT IN A SALT-LOSING DISORDER. J Clin Endocrinol Metab. 1964 Jul;24:669–672. doi: 10.1210/jcem-24-7-669. [DOI] [PubMed] [Google Scholar]
- VISSER H. K., COST W. S. A NEW HEREDITARY DEFECT IN THE BIOSYNTHESIS OF ALDOSTERONE: URINARY C21-CORTICOSTEROID PATTERN IN THREE RELATED PATIENTS WITH A SALT-LOSING SYNDROME, SUGGESTING AN 18-OXIDATION DEFECT. Acta Endocrinol (Copenh) 1964 Dec;47:589–612. doi: 10.1530/acta.0.0470589. [DOI] [PubMed] [Google Scholar]