

Abstract
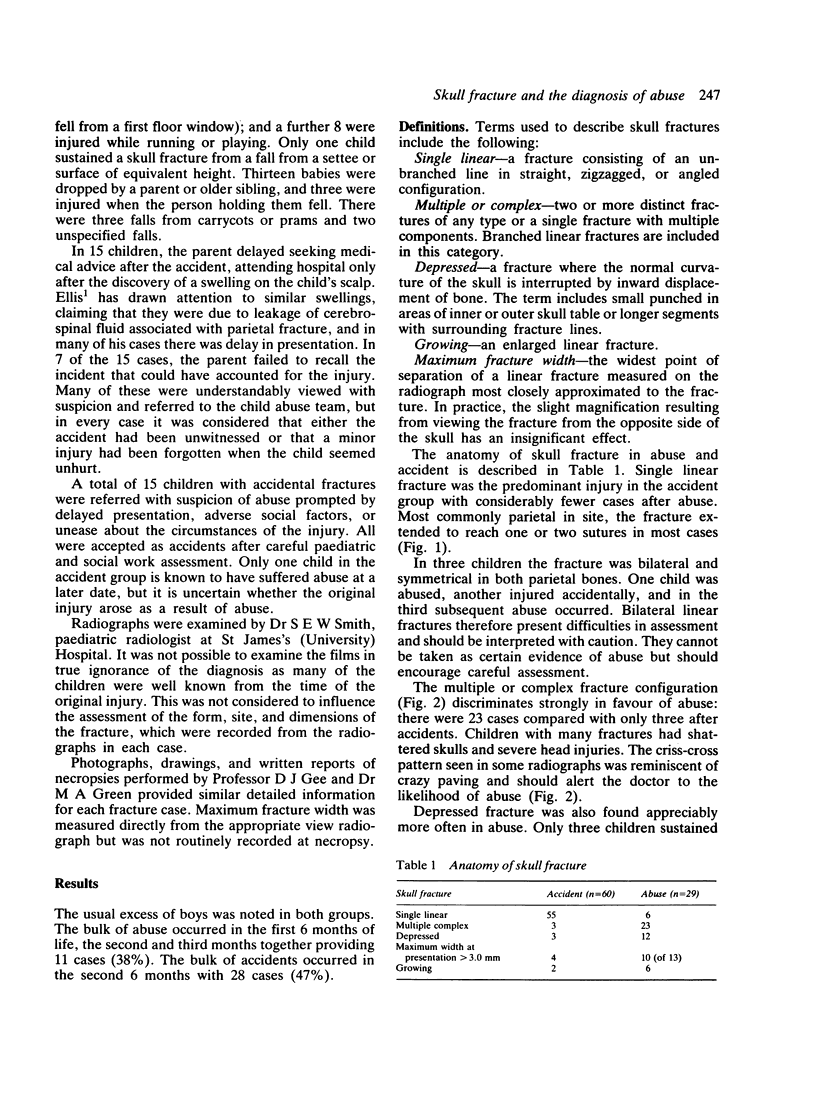
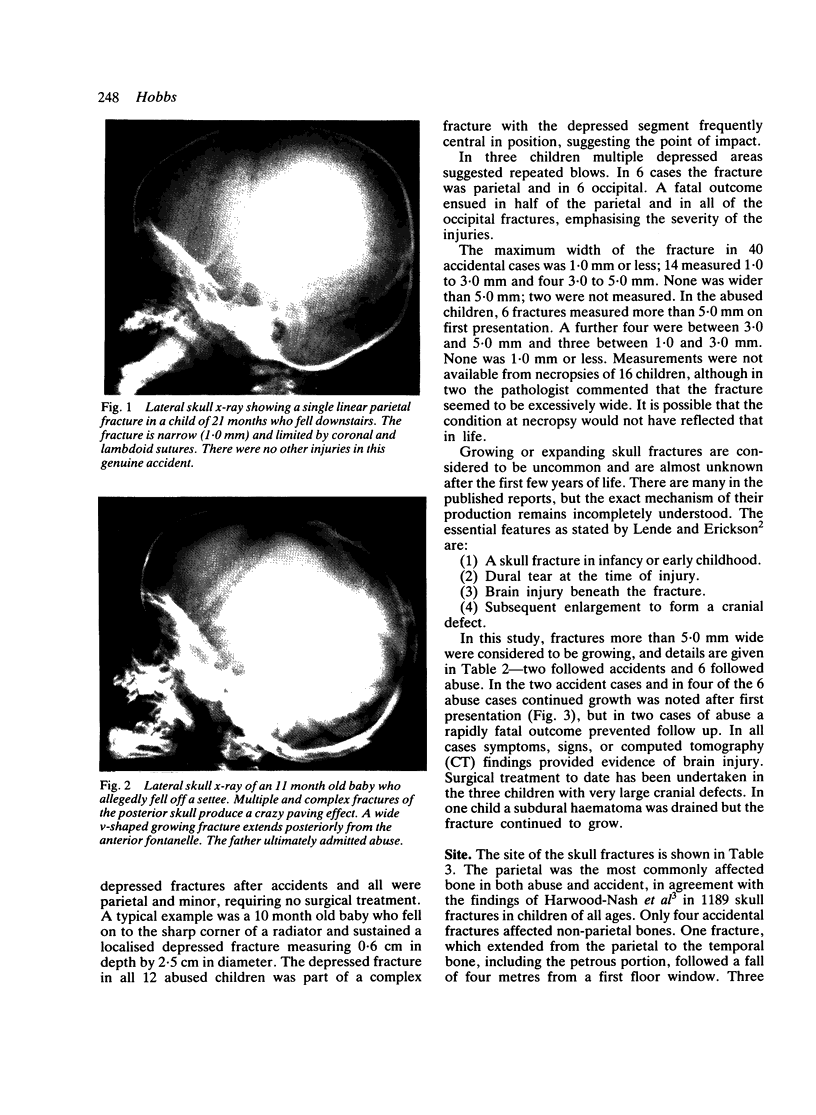
Eighty nine children under 2 years of age with skull fracture were studied retrospectively--29 children with definite non-accidental injury serially recorded by the Departments of Paediatrics and Forensic Medicine, and 60 children consecutively admitted to hospital with skull fractures after accidents. There were 20 deaths including 19 among abused children. Multiple injuries and an inadequate history assisted in diagnosing abuse. Fracture characteristics found considerably more often in abused children were: multiple or complex configuration; depressed, wide, and growing fracture; involvement of more than a single cranial bone; non-parietal fracture; and associated intracranial injury including subdural haematoma. No fractures measuring more than 5.0 mm on presentation were found after accidents, but 6 of these 'growing fractures' were found in abused children. Accidents usually resulted in single, narrow, linear fractures most commonly of the parietal, with no associated intracranial injury. The results suggest that in skull fracture in young children where a minor fall is alleged, it is possible to recognise abuse by consideration of the fracture alone.
Full text
PDF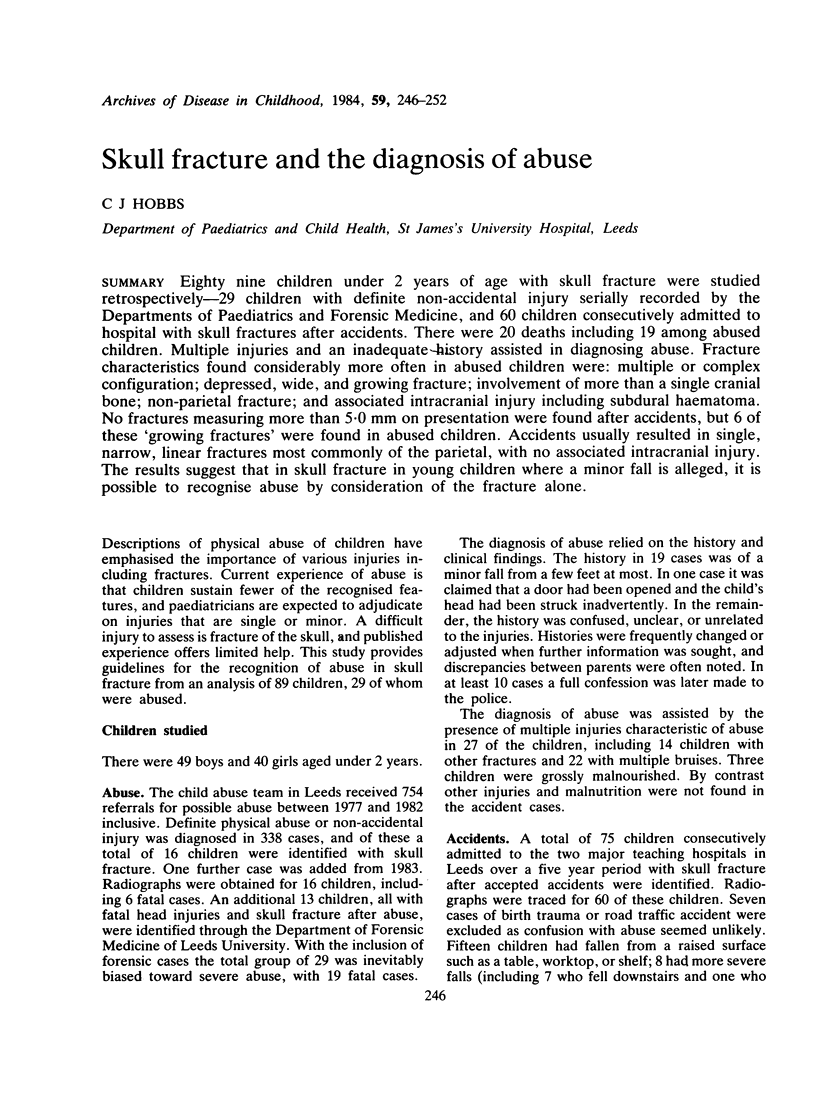
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ELLIS M. Fractures of the parietal bone in children. Lancet. 1958 May 17;1(7029):1048–1049. doi: 10.1016/s0140-6736(58)92009-9. [DOI] [PubMed] [Google Scholar]
- Harwood-Nash D. C., Hendrick E. B., Hudson A. R. The significance of skull fractures in children. A study of 1,187 patients. Radiology. 1971 Oct;101(1):151–156. doi: 10.1148/101.1.151. [DOI] [PubMed] [Google Scholar]
- Helfer R. E., Slovis T. L., Black M. Injuries resulting when small children fall out of bed. Pediatrics. 1977 Oct;60(4):533–535. [PubMed] [Google Scholar]
- Kingsley D., Till K., Hoare R. Growing fractures of the skull. J Neurol Neurosurg Psychiatry. 1978 Apr;41(4):312–318. doi: 10.1136/jnnp.41.4.312. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kuhns L. R., Nelson D., Deibert G. Transillumination detection of a growing skull fracture. Am J Dis Child. 1977 Aug;131(8):889–892. doi: 10.1001/archpedi.1977.02120210067014. [DOI] [PubMed] [Google Scholar]
- LENDE R. A., ERICKSON T. C. Growing skull fractures of childhood. J Neurosurg. 1961 Jul;18:479–489. doi: 10.3171/jns.1961.18.4.0479. [DOI] [PubMed] [Google Scholar]
- Meyer H. M., Jr, Parkman P. D., Hopps H. E. The control of rubella. Pediatrics. 1969 Jul;44(1):5–20. [PubMed] [Google Scholar]
- Rothman L., Rose J. S., Laster D. W., Quencer R., Tenner M. The spectrum of growing skull fracture in children. Pediatrics. 1976 Jan;57(1):26–31. [PubMed] [Google Scholar]
- Stein B. M., Tenner M. S. Enlargement of skull fracture in childhood due to cerebral herniation. Arch Neurol. 1972 Feb;26(2):137–143. doi: 10.1001/archneur.1972.00490080055005. [DOI] [PubMed] [Google Scholar]
- TAVERAS J. M., RANSOHOFF J. Leptomeningeal cysts of the brain following trauma with erosion of the skull; a study of seven cases treated by surgery. J Neurosurg. 1953 May;10(3):233–241. doi: 10.3171/jns.1953.10.3.0233. [DOI] [PubMed] [Google Scholar]
- Thompson J. B., Mason T. H., Haines G. L., Cassidy R. J. Surgical management of diastatic linear skull fractures in infants. J Neurosurg. 1973 Oct;39(4):493–497. doi: 10.3171/jns.1973.39.4.0493. [DOI] [PubMed] [Google Scholar]
- Vas C. J., Winn J. M. Growing skull fractures. Dev Med Child Neurol. 1966 Dec;8(6):735–740. doi: 10.1111/j.1469-8749.1966.tb01834.x. [DOI] [PubMed] [Google Scholar]