

Abstract
The introduction of topical calcineurin inhibitors resulted in a significant improvement in the treatment of atopic dermatitis. In addition, rapid amelioration of pruritus could be observed. In case reports, other pruritic dermatoses such as chronic irritative hand dermatitis, rosacea, graft-versus-host-disease, and lichen sclerosus were also treated successfully with pimecrolimus and tacrolimus. Twenty patients were treated with tacrolimus and pimecrolimus in a surveillance study to evaluate efficacy in pruritus and prurigo. Eighteen of 20 patients responded to therapy. Best results were obtained in localized and generalized pruritus while in prurigo nodularis only a subgroup of patients showed an improvement of pruritus. Further controlled studies are necessary to confirm these results.
Keywords: Pimecrolimus, tacrolimus, pruritus, itch, vanilloid receptor
Introduction
Chronic pruritus is frequently resistant to common therapeutic regimens and demands new approaches (Ständer, Steinhoff, Schmelz, et al 2003; Weisshaar et al 2003). Therefore, the current neurophysiological and neuromorphological research (Ständer, Steinhoff, Schmelz, et al 2003; Greaves and Khalifa 2004) focuses on this problem. Up to now, it is known that pruritus can be evoked by mediators such as histamine, neuropeptides, proteinases, prostaglandins, serotonin, and bradykinin (Schmelz 2002; Ständer, Steinhoff, Schmelz, et al 2003). Moreover, current investigations identified new receptor systems on cutaneous sensory nerve fibers such as vanilloid, opioid, and cannabinoid receptors that can modulate itch and thereby represent targets for antipuritic therapy (Ständer et al 2002, 2004, 2005). Interestingly, the vanilloid receptor TRPV1 induces burning itch upon short-term activation while chronic stimulation leads to the interruption of nociceptive transmission to the central nervous system (Caterina et al 1997; Ständer et al 2001). In current studies there is indirect evidence that next to capsaicin also the calcineurin inhibitors may bind to the TRPV1 (Ständer, Steinhoff, Ständer, et al 2003; Senba et al 2004). Based on this theory, it may be speculated that pimecrolimus and tacrolimus may not only suppress pruritus in atopic dermatitis but also in other pruritic diseases. In this paper we report for the first time on the efficacy of topical calcineurin inhibitors in diseases such as prurigo nodularis, generalized and localized pruritus including genitoanal pruritus. 20 patients (12 female, 8 male; 26 to 76 years, mean age 55.9 years) with generalized (n = 3) and localized (n = 2; lower legs, n = 1; back, n = 1) pruritus, pruritus of the genitoanal area (n = 4; scrotal, n = 2; vulva, n = 1; anal, n = 1), and prurigo nodularis (n = 11) were treated with pimecrolimus 1% cream and tacrolimus 0.1% ointment. Patients had been suffering from pruritus since 5 months up to 20 years (mean, 4.2 years; 5 months, n = 1; 6 months, n = 2; 11 months, n = 1; 1 year, n = 2; 18 months, n = 1; 20 months, n = 1; 22 months, n = 1; 2 years, n = 3; 3 years, n = 2; 4 years, n = 1; 5 years, n = 1; 10 years, n = 2; 14 years, n = 1; 20 years, n = 1).
Table 1.
Antipruritic effect in chronic pruritus and prurigo: patients, applied calcineurin inhibitor, and outcome
| Age, sex | Diagnosis/duration of disease | Type of calcineurin inhibitor | Duration of therapy | Antipruritic effect in percent reduction of itch | Influence on skin lesions |
|---|---|---|---|---|---|
| Pruritus | |||||
| 52 years, male | Generalized pruritus/since 10 years | Tacrolimus 0.1% | 11 months | 70% reduction | None present |
| 74 years, male | Generalized pruritus/10 years | Pimecrolimus 1% | 3 months | 50% reduction | None present |
| 69 years, female | Generalized pruritus/2 years | Pimecrolimus 1% | 14 days | 90% reduction | None present |
| 37 years, male | Pruritus lower legs/4 years | Pimecrolimus 1% | 1 month | 100% reduction | None present |
| 76 years, female | Pruritus on the back/1 year | Pimecrolimus 1% | 1 month | 50% reduction | None present |
| Genitoanal pruritus | |||||
| 63 years, male | Genital pruritus/6 months | Tacrolimus 0.1% | 7 months | 100% reduction | None present |
| 31 years, female | Genital pruritus with lichen simplex/14 years | Pimecrolimus 1% | 24 months | 100% reduction | Healing* |
| 72 years, male | Scrotal pruritus/2 years | Pimecrolimus 1% | 6 months | 100% reduction | None present |
| 39 years, male | Anal pruritus/1 year | Pimecrolimus 1% | 1 month | 100% reduction | None present |
| Prurigo nodularis | |||||
| 28 years, female | Prurigo nodularis/5 years | Tacrolimus 0.1% | 3 months | 100% reduction | Healing |
| 74 years, female | Prurigo nodularis/6 months | Pimecrolimus 1% | 16 months | 100% reduction | Healing |
| 63 years, female | Prurigo nodularis/20 years | Pimecrolimus 1% | 5 months | 100% reduction | Healing |
| 54 years, male | Prurigo nodularis/20 months | Pimecrolimus 1% | 25 months | 70% reduction | Improvement |
| 54 years, female | Prurigo nodularis/22 months | Pimecrolimus 1% | 7 months | 70% reduction | Improvement |
| 74 years, female | Prurigo nodularis/2 years | Pimecrolimus 1% | 6 months | 50% reduction | Improvement |
| 51 years, female | Prurigo nodularis/11 months | Tacrolimus 0.1% | 3 weeks | 50% reduction | Improvement |
| 48 years, female | Prurigo nodularis/3 years | Pimecrolimus 1% | 3 weeks | 20% reduction | Minor improvement* |
| 26 years, female | Prurigo nodularis/5 months | Tacrolimus 0.1% | 2 months | 20% reduction | Minor improvement |
| 73 years, male | Prurigo nodularis/18 months | Pimecrolimus 1% | 8 days | No response | No response |
| 55 years, female | Prurigo nodularis/3 years | Tacrolimus 0.1% | 3 weeks | No response | No response |
Improvement: healing between 50% to 70% of skin lesions, minor improvement: healing up to 50% of skin lesions
The underlying origin could be identified in 12 patients: a combination (5 patients) or single (7 patients) presence of psychogenic factors (n = 5), deficiency of vitamins (n = 6, iron, n = 1; zinc, n = 4; and vitamin B12, n = 1), helicobacter infection of the stomach (n = 2), diabetes mellitus (n = 1), xerosis in elderly (n = 2), atopic predisposition (n = 6; without atopic eczema) led to the itch. In 8 patients, no underlying cause could be identified. The intense and chronic pruritus leads in 11 patients to the clinical picture of prurigo nodularis with flat or prominent erosive and crusted papules and nodules. All patients with localized, generalized, and genitoanal pruritus had no or minimal linear scratch lesions, except of one female patient with lichenification in the genial area.
Pruritus was therapy refractory to topical (n = 14) and systemical corticosteroids (n = 3), antihistamines (n = 9), UV-therapy (n = 8), moisturing the skin (n = 5), capsaicin (n = 2), opiate receptor antagonists (n = 1), serotonin reuptake inhibitors (n = 1), antiparasital and antifungal therapies (n = 6).
All patients received topical calcineurin inhibitors in an open uncontrolled surveillance study. All patients were informed about pimecrolimus and tacrolimus and that they are already commercially available for atopic dermatitis. Patients applied the topical twice daily; no other topical or systemical antipruritic therapy was allowed. As according to the current literature most patients were treated for pruritus with tacrolimus, we applied tacrolimus in 6 patients only while 14 were treated with pimecrolimus. In each diagnosis group, at least one patient was treated with tacrolimus to control that pruritus responds to this substance. In the large group of prurigo nodularis, 4 patients with different stage of the disease received tacrolimus. The patients were seen every 4 weeks and were investigated clinically for presence and expansion of skin lesions. The antipruritic effect was evaluated as follows: the itch intensity before starting therapy was rated as 100%. Then all patients were asked to quote the itch reduction in percent during the therapy (eg, if itch intensity was reduced about half, it was scored as 50% itch reduction). In prurigo nodularis, photographic documentation was performed.
Figure 1.
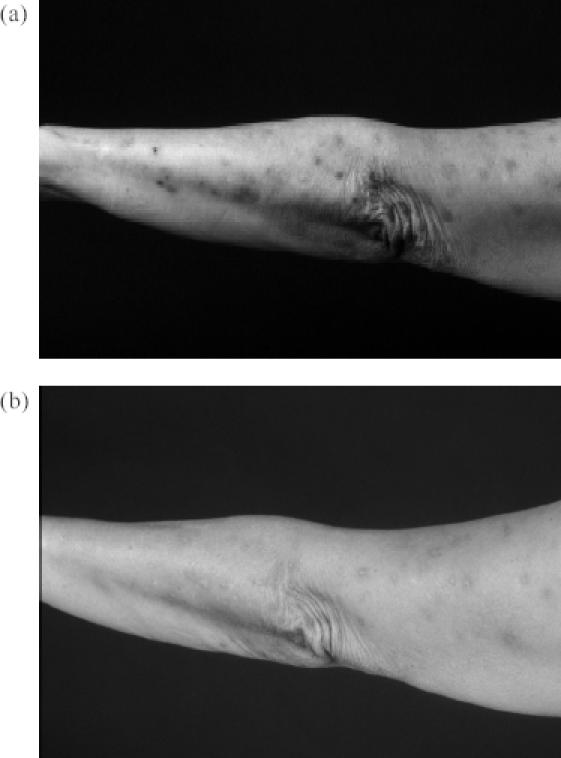
Female 74-year old patient with prurigo nodularis since 6 months (a). After a therapy of 12 months all lesions of the arm cleared (b).
Results
Eighteen of the 20 patients responded to therapy; 2 patients (10%) did not report any antipruritic effect. A complete reduction of itch (100% itch reduction) was achieved in 8 patients (40%); an almost complete cessation (70% itch reduction, n = 3; 90% itch reduction, n=1) was observed in 4 patients (20%). An itch reduction of 50% was reported by 4 patients (20%) while 2 patients (10%) showed almost no improvement of itch (20% itch reduction). The mean itch reduction in all patients was 67%.
Best response was achieved in genitoanal pruritus. All patients experienced a complete reduction of pruritus using pimecrolimus (n = 3) or tacrolimus (n = 1). Patients reported a rapid cessation of itch within the initial three days of treatment. In a patient with additional lichenification due to chronic scratching, all lesions resolved.
In generalized and localized pruritus, a good reduction of pruritus was observed (mean itch reduction: 72%). Three of 5 patients responded with complete (n = 1) or nearly complete (n = 2) relief of itch. Pruritus was reduced to 50% in additional 2 patients. These results were similar in using tacrolimus or pimecrolimus; tacrolimus achieved a reduction of 70% in one patient; pimecrolimus a mean reduction of 72.5% in 4 patients. In prurigo nodularis, a complete relief (100%) or almost complete cessation (70%) of itch and healing or major improvement of the lesions was achieved in 5 patients (tacrolimus, n = 1; pimecrolimus, n = 4). In 2 other patients, tacrolimus and pimecrolimus achieved a 50% reduction of itch, respectively. In 4 other patients, both calcineurin inhibitors showed only weak (20%, n = 2) or no (n = 2) antipruritic effect without improvement of skin lesions. The average itch reduction in prurigo nodularis was 53%.
Pimecrolimus and tacrolimus were applied individually up to the maximal achievable relief of the itch and clearance of all skin lesions. The duration of therapy varied from 14 days to 11 months (mean, 7.3 months; 14 days, n = 1; 3 weeks, n = 1; 1 month, n = 3; 3 months, n = 2; 5 months, n = 1; 6 months, n = 2; 7 months, n = 2; 11 months, n = 1; 16 months, n = 1, 2 years, n = 2). In the group of no or weak response (up to 30% pruritus reduction and less), therapy was stopped after 8 days (n = 1), 3 weeks (n = 2), or 2 months (n = 1).
All patients with application of the calcineurin inhibitors in the genital area reported an intense burning in the first two to three days. After these initial days the burning stops. In the other two groups, only single patients treated with either pimecrolimus or tacrolimus complained on initial burning. No other side effects appear.
Discussion
The development of topical calcineurin inhibitors resulted in a significant improvement in the treatment of atopic dermatitis (Simpson and Noble 2005). Parallel to the rapid reduction of eczematous lesions, fast relief of pruritus was observed (Meurer et al 2002; Reitamo et al 2002; Ständer and Luger 2003). The antipruritic effect is currently believed to be related to the inhibition of inflammatory cytokines (Bornhövd et al 2002). Pimecrolimus and tacrolimus primarily induce calcineurin inhibition that interrupts cytokine gene expression and leads to the down regulation of T-cell activity. Furthermore, recent investigations suggest that calcineurin inhibitors may also directly influence nerve fiber function by possible binding to a receptor on small, unmyelinated sensory nerve fibers, the TRPV1 (VR1, capsaicin receptor) (Ständer, Steinhoff, Ständer, et al 2003; Senba et al 2004). After activation of this receptor eg, by capsaicin, nerve fibers are depolarized resulting in transmission of burning pain and itch and the release of neuropeptides. Along with continuous stimulation of the TRPV1, the receptor is finally desensitized and the transmission of nociceptive stimuli is inhibited. These findings may provide a possible explanation for the observed calcineurin inhibitors-related side-effects such as initial burning and pruritus, and moreover, the following rapid reduction of pruritus.
Previously, a complete relief of pruritus under twice daily topical tacrolimus 0.1% therapy was reported in a patient with severe pruritus induced by primary biliary cirrhosis (Aguilar-Bernier et al 2005) (Table 2). Tacrolimus application in uremic pruritus led to conflicting results. While in a case report with single patients (Pauli-Magnus et al 2000) and in a prospective study with two sequential concentrations of tacrolimus (0.03%, 0.1%) ointment (Kuypers et al 2004) this substance led to significant reduction of itch in uremic pruritus, a randomized, double-blind, vehicle-controlled study did not demonstrate that tacrolimus ointment 0.1% is more effective than its vehicle in relieving uremic pruritus (Duque et al 2005).
Table 2.
Antipruritic effect of calcineurin inhibitors in pruritic diseases reported in case reports, case series, uncontrolled, and controlled studies
| Author | Diagnosis | Number of patients | Topical Immunomodulator | Reduction of itch |
|---|---|---|---|---|
| Aguilar-Bernier et al 2005 | Pruritus in primary biliary cirrhosis | 1 | Tacrolimus 0.1%, twice daily | 100% relief within 1 month, QoL improved |
| Pauli-Magnus et al 2000 | Uremic pruritus | 3 | Tacrolimus 0.03%, twice daily | 100% relief within 2 days |
| Cherill et al 2000 | Chronic-irritative hand eczema | 48 | Pimecrolimus 1% | Significant reduction |
| Goldman 2001 | Steroid-induced rosacea | 3 | Tacrolimus 0.075% | 100% relief within 7 to 10 days |
| Choi and Nghiem, 2001 | Chronic GvhD | 18 | Tacrolimus 0.1% | Reduction in 13 patients |
| Böhm et al 2003 | Genitoanal lichen sclerosus et atrophicus | 3 children (5–9 years) 3 adults | Tacrolimus 0.1% | Significant reduction within 8 days |
| Banky et al 2004 | Epidermolysis bullosa pruriginosa | 1 | Tacrolimus 0.03%, twice daily | 100% relief within 1 week, scratch marks reduced |
| Kuypers et al 2004 | Uremic pruritus | 21 | Tacrolimus 0.1% (3 weeks) then 0.03% (3 weeks), twice daily | 81.8% reduction within 6 weeks |
| Duque et al 2005 | Uremic pruritus | 20 (12 with tacrolimus, 8 received vehicle) | Tacrolimus 0.1%, twice daily | 100% relief in tacrolimus and vehicle group |
Abbreviations: GvhD, graft versus host disease; QoL, quality of life.
Several reports also demonstrate the antipruritic efficacy of the topical immunomodulators in dermatological diseases. For example, a patient with epidermolysis bullosa pruriginosa was treated with tacrolimus 0.03% for otherwise intractable itching on the legs and experienced a relief within one week (Banky et al 2004). Patients with chronic irritative hand dermatitis experienced significant reduction of itch during topical treatment with pimecrolimus 1% (Cherill et al 2000). In pruritus of steroid-induced rosacea (Goldmann 2001), chronic graft-versus-host-disease (Choi and Nghiem 2001), and lichen sclerosus et atrophicus (Böhm et al 2003), case reports demonstrated antipruritic efficacy of tacrolimus 0.075%–0.1% therapy within 7 to 10 days (Table 2).
In the current surveillance study, the antipruritic potency of calcineurin inhibitors in prurigo nodularis, generalized and localized pruritus including genitoanal pruritus was evaluated. Since most of the previous reports demonstrated convincing antipruritic effects of tacrolimus application, we focussed on topical pimecrolimus therapy. All investigated diagnoses showed a response to topical therapy with tacrolimus and pimecrolimus. A continuous significant antipruritic effect was obtained in genitoanal pruritus with either tacrolimus or pimecrolimus. Patients reported on fast reduction of itch (after 2 to 3 days) after cessation of initial burning. Genitoanal pruritus is a frequent, localized form of pruritus mostly induced by infections (eg, candidiasis), helminths, hemorrhoids, or genital dermatological diseases such as psoriasis and atopic dermatitis (Welsh et al 2004; Eichmann 2005). Though the underlying origin may frequently be identified, therapy is difficult due to the increased resorption and sensitivity in this area. Due to our findings, topical calcineurin inhibitors may be a safe treatment alternative. Also, other types of localized and generalized pruritus of unknown origin without primary skin lesions could be influenced by topical calcineurin inhibitors. However, the efficacy of therapy varied from 50% to 100% concerning the reduction of the pruritus. Interestingly, in a patient with xerosis and beginning exsiccation dermatitis, an almost complete reduction (90% itch reduction) was achieved.
Figure 2.
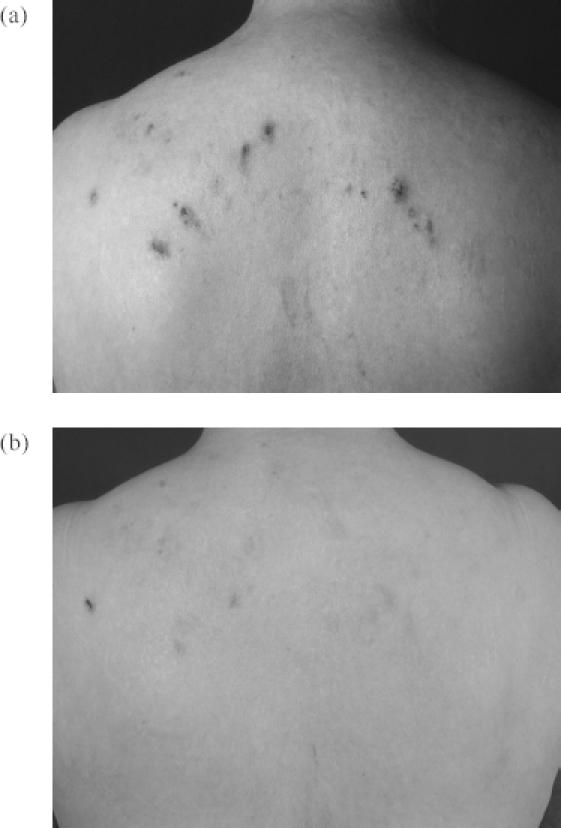
Female 63-year-old patient with prurigo nodularis since 20 years (a). After a 5 months therapy all skin lesions cleared and skin remained stable after one month stopping the treatment (b).
Prurigo nodularis is not an own entity but a descriptive term for chronic secondary scratch lesions due to therapy refractory pruritus. In our patients, pruritus was induced by mainly psychogenic and internal diseases and less by cutaneous disorders. According to the severity of prurigo nodularis, both calcineurin inhibitors achieved a significant improvement of pruritus and skin lesions consisting of papules and flat nodules. Thick nodules did not respond to this therapy which is most likely due to decreased penetration of the active substance. These results suggest that calcineurin inhibitors may be helpful in a subgroup of patients with prurigo nodularis. Further studies with larger collectives of patients have to evaluate the efficacy of tacrolimus and pimecrolimus in prurigo nodularis.
References
- Aguilar-Bernier M, Bassas-Vila J, Sanz-Munoz C, et al. Successful treatment of pruritus with topical tacrolimus in a patient with primary biliary cirrhosis. Br J Dermatol. 2005;152:808–9. doi: 10.1111/j.1365-2133.2005.06498.x. [DOI] [PubMed] [Google Scholar]
- Banky JP, Sheridan AT, Storer EL, et al. Successful treatment of epidermolysis bullosa pruriginosa with topical tacrolimus. Arch Dermatol. 2004;140:794–6. doi: 10.1001/archderm.140.7.794. [DOI] [PubMed] [Google Scholar]
- Böhm M, Frieling U, Luger TA, et al. Successful treatment of anogenital lichen sclerosus with topical tacrolimus. Arch Dermatol. 2003;139:922–4. doi: 10.1001/archderm.139.7.922. [DOI] [PubMed] [Google Scholar]
- Bornhövd EC, Burgdorf WH, Wollenberg A. Immunomodulatory macrolactams for topical treatment of inflammatory skin diseases. Curr Opin Investig Drugs. 2002;3:708–12. [PubMed] [Google Scholar]
- Caterina MJ, Schumacher MA, Tominaga M, et al. The capsaicin receptor: a heat-activated ion channel in the pain pathway. Nature. 1997;389:816–24. doi: 10.1038/39807. [DOI] [PubMed] [Google Scholar]
- Cherill R, Tofte S, MacNaul R, et al. SDZ ASM 981 1% cream is effective in the treatment of chronic irritant hand dermatitis. J Eur Acad Dermatol Venereol. 2000;14(Suppl 1):128. [Google Scholar]
- Choi CJ, Nghiem P. Tacrolimus ointment in the treatment of chronic cutaneous graft-vs-host disease: a case series of 18 patients. Arch Dermatol. 2001;137:1202–6. doi: 10.1001/archderm.137.9.1202. [DOI] [PubMed] [Google Scholar]
- Duque MI, Yosipovitch G, Fleischer AB, Jr, et al. Lack of efficacy of tacrolimus ointment 0.1% for treatment of hemodialysis-related pruritus: a randomized, double-blind, vehicle-controlled study. J Am Acad Dermatol. 2005;52:519–21. doi: 10.1016/j.jaad.2004.08.050. [DOI] [PubMed] [Google Scholar]
- Eichmann AR. Dermatoses of the male genital area. Dermatology. 2005;210:150–6. doi: 10.1159/000082571. [DOI] [PubMed] [Google Scholar]
- Goldman D. Tacrolimus ointment for the treatment of steroid-induced rosacea: a preliminary report. J Am Acad Dermatol. 2001;44:995–8. doi: 10.1067/mjd.2001.114739. [DOI] [PubMed] [Google Scholar]
- Greaves MW, Khalifa N. Itch: more than skin deep. Int Arch Allergy Immunol. 2004;135:166–72. doi: 10.1159/000080898. [DOI] [PubMed] [Google Scholar]
- Kuypers DR, Claes K, Evenepoel P, et al. A prospective proof of concept study of the efficacy of tacrolimus ointment on uraemic pruritus (UP) in patients on chronic dialysis therapy. Nephrol Dial Transplant. 2004;19:1895–901. doi: 10.1093/ndt/gfh202. [DOI] [PubMed] [Google Scholar]
- Meurer M, Fölster-Holst R, Wozel G, et al. Pimecrolimus cream in the long-term management of atopic dermatitis in adults: a six-month study. Dermatology. 2002;205:271–7. doi: 10.1159/000065863. [DOI] [PubMed] [Google Scholar]
- Pauli-Magnus C, Klumpp S, Alscher DM, et al. Short-term efficacy of tacrolimus ointment in severe uremic pruritus. Perit Dial Int. 2000;20:802–3. [PubMed] [Google Scholar]
- Reitamo S, Van Leent EJ, Ho V, et al. Efficacy and safety of tacrolimus ointment compared with that of hydrocortisone acetate ointment in children with atopic dermatitis. J Allergy Clin Immunol. 2002;109:539–46. doi: 10.1067/mai.2002.121831. [DOI] [PubMed] [Google Scholar]
- Schmelz M. Itch – mediators and mechanisms. J Dermatol Sci. 2002;28:91–6. doi: 10.1016/s0923-1811(01)00167-0. [DOI] [PubMed] [Google Scholar]
- Senba E, Katanosaka K, Yajima H, et al. The immunosuppressant FK506 activates capsaicin- and bradykinin-sensitive DRG neurons and cutaneous C-fibers. Neurosci Res. 2004;50:257–62. doi: 10.1016/j.neures.2004.07.005. [DOI] [PubMed] [Google Scholar]
- Simpson D, Noble S. Tacrolimus ointment: a review of its use in atopic dermatitis and its clinical potential in other inflammatory skin conditions. Drugs. 2005;65:827–58. doi: 10.2165/00003495-200565060-00011. [DOI] [PubMed] [Google Scholar]
- Ständer S, Luger T, Metze D. Treatment of prurigo nodularis with topical capsaicin. J Am Acad Dermatol. 2001;44:471–8. doi: 10.1067/mjd.2001.110059. [DOI] [PubMed] [Google Scholar]
- Ständer S, Gunzer M, Metze D, et al. Localization of mu-opioid receptor 1A on sensory nerve fibers in human skin. Regul Pept. 2002;110:75–83. doi: 10.1016/s0167-0115(02)00159-3. [DOI] [PubMed] [Google Scholar]
- Ständer S, Steinhoff M, Ständer H, et al. Morphological evidence of neuropeptide release and mast cell degranulation in tacrolimus (FK 506) and pimecrolimus (SDZ ASM 981) treated murine skin [abstract] J Invest Dermatol. 2003;121:0912. [Google Scholar]
- Ständer S, Steinhoff M, Schmelz M, et al. Neurophysiology of pruritus: cutaneous elicitation of itch. Arch Dermatol. 2003;139:1463–70. doi: 10.1001/archderm.139.11.1463. [DOI] [PubMed] [Google Scholar]
- Ständer S, Luger TA. Antipruritic effects of pimecrolimus and tacrolimus. Hautarzt. 2003;54:413–17. doi: 10.1007/s00105-003-0521-6. [DOI] [PubMed] [Google Scholar]
- Ständer S, Moormann C, Schumacher M, et al. Expression of vanilloid receptor subtype 1 in cutaneous sensory nerve fibers, mast cells, and epithelial cells of appendage structures. Exp Dermatol. 2004;13:129–39. doi: 10.1111/j.0906-6705.2004.0178.x. [DOI] [PubMed] [Google Scholar]
- Ständer S, Schmelz M, Metze D, et al. Distribution of cannabinoid receptor 1 (CB1) and 2 (CB2) on sensory nerve fibers and adnexal structures in human skin. J Dermatol Sci. 2005;38:177–88. doi: 10.1016/j.jdermsci.2005.01.007. [DOI] [PubMed] [Google Scholar]
- Weisshaar E, Kucenic MJ, Fleischer AB., Jr Pruritus: A review. Acta Derm Venereol Suppl (Stockh) 2003;213:5–32. [PubMed] [Google Scholar]
- Welsh B, Howard A, Cook K. Vulval itch. Aust Fam Physician. 2004;33:505–10. [PubMed] [Google Scholar]