
Figure 1 .
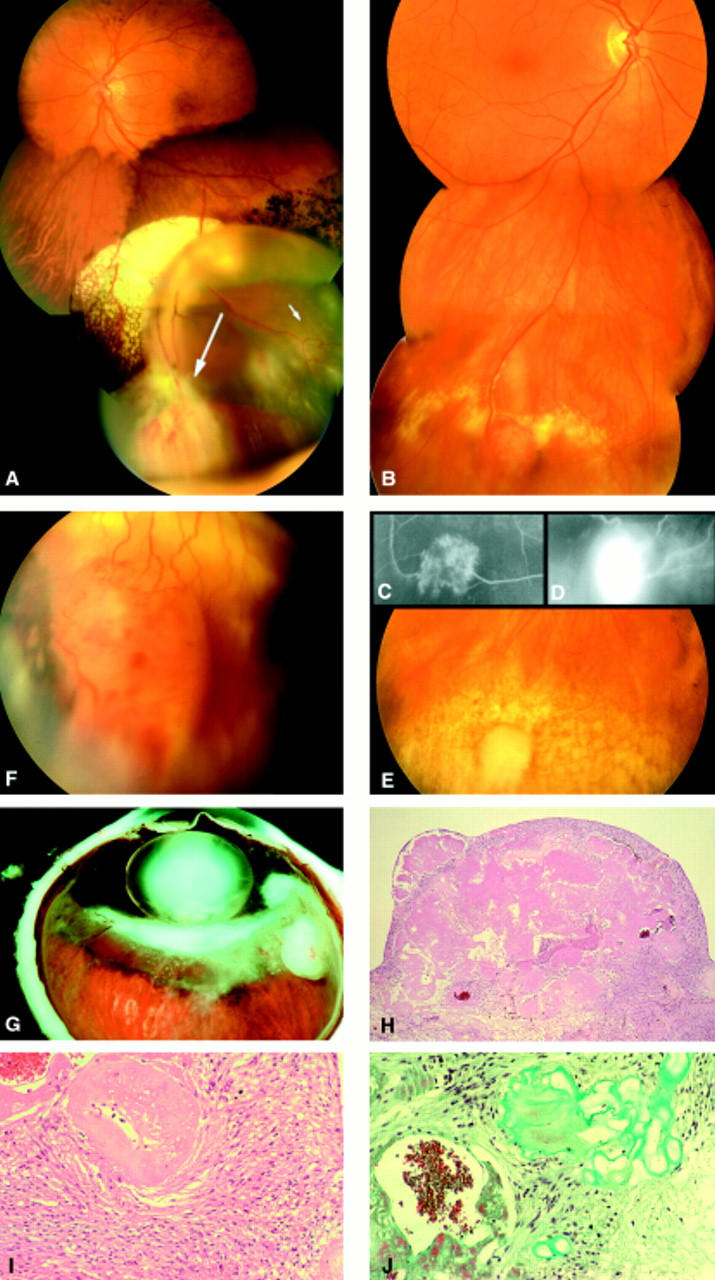
(A) VPTR in the lower retinal periphery in a 31 year old male patient who presented with floaters and loss of vision. The tumour (long arrow) is accompanied by an exudative retinal detachment, intraretinal accumulations of lipoid exudates, telangiectactic alterations of the retinal vessels (small arrow), and marked hyperpigmentations of the retinal pigment epithelium in the retina adjacent to the exudative detachment. (B) Symptomless VPTR in the lower retinal periphery in a 65 year old female patient. (C) Mid-phase fluorescein angiography of the tumour shown in (B) demonstrating the connection of tumour vessels with non-dilated retinal vessels. (D) Late phase fluorescein angiography of the tumour shown in (B) demonstrating preretinal leakage of dye on the tumour surface. (E) VPTR as shown in (B, C) 6 months after brachytherapy with 106-ruthenium. Regression of tumour thickness and exudative retinal changes. Chorioretinal scarring within the area that was covered by the 106-ruthenium plaque. (F) VPTR in the lower retinal periphery of a 15 year old boy with a history of toxoplasmosis retinochoroiditis. (G) Enucleation specimen with VPTR of the retinal periphery in a 27 year old male patient who presented with a blind and painful eye as a result of neovascular glaucoma. (H) Low power magnification of the retinal tumour demonstrating that it consists of a proliferation of glial cells and small blood vessels embedded in a hyalinised stromal matrix (haematoxylin and eosin stain, ×10 objective). (I) High power magnification of a hyalinised blood vessel surrounded by glial cells (haematoxylin and eosin stain, ×40 objective). (J) High power magnification of a blood vessel filled with erythrocytes and surrounded by glial cells and hyalinised stroma (Gomori stain, ×40 objective). (A and B were assembled using digitised fundus photographs and Adobe Photoshop software).