
Figure 1 .
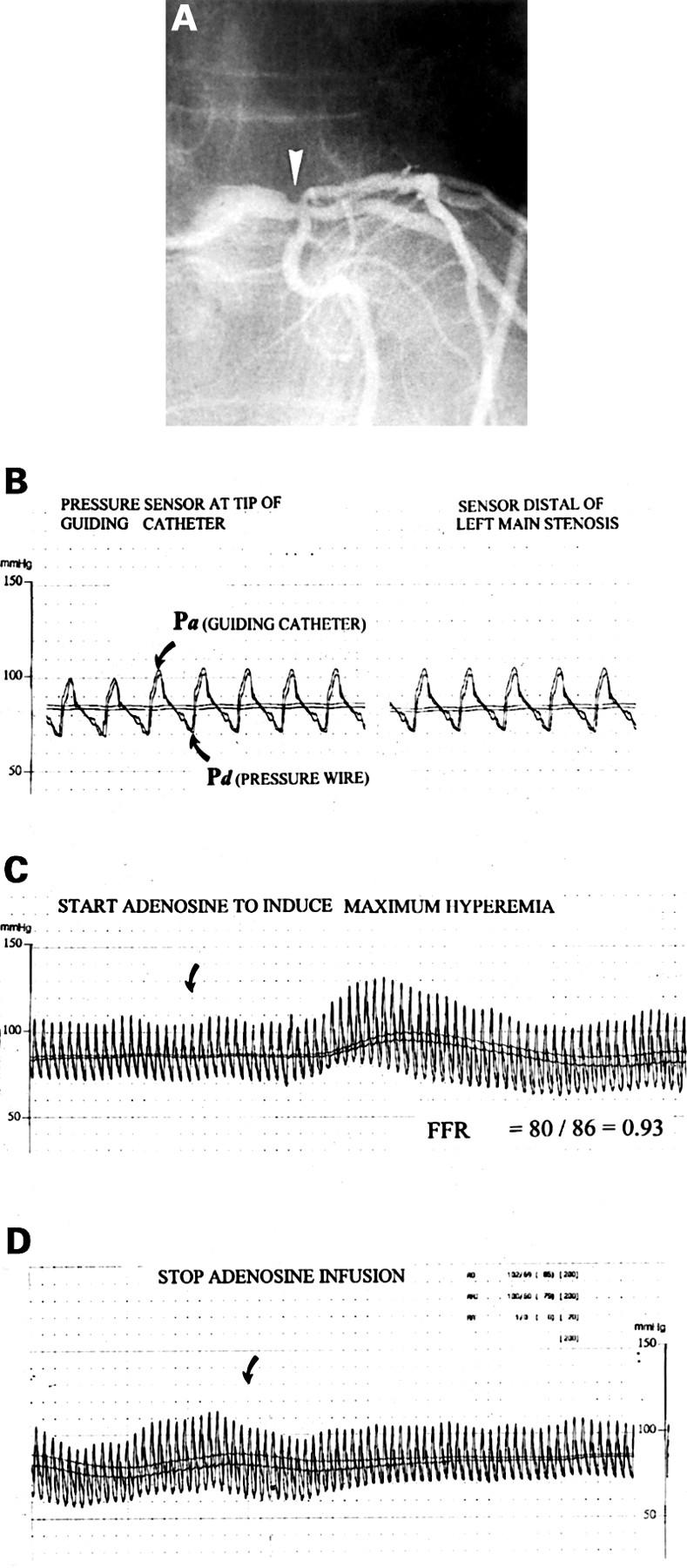
(A) Coronary angiogram in the right anterior oblique projection of a 58 year old man with anginal complaints, a reversible defect on exercise perfusion scintigraphy in the anterior wall, a 40% stenosis (arrow) at the transition of the distal left main coronary artery (LM), and an 80% stenosis of the proximal left anterior descending coronary artery (LAD). The dilemma was to decide whether the ischaemia was caused by the proximal LAD disease only or also by the left main stenosis, and consequently if bypass surgery should be performed or only percutaneous transluminal coronary angioplasty (PTCA) of the proximal LAD. (B) Paper speed is 25 mm/s. The pressure wire is advanced until the sensor is close to the tip of the guiding catheter to confirm that two identical signals are obtained. Pa is the pressure as measured by the guiding catheter and Pd the pressure as measured by the pressure wire. The pressure wire is then advanced across the LM stenosis into the large intermediate branch and no gradient is observed at rest. (C) Paper speed is 5 mm/s. About 20 seconds after the start of the intravenous adenosine infusion (140 µg/kg/min) a pressure gradient gradually develops (arrow) and at steady state, maximum coronary hyperaemic myocardial fractional flow reserve is calculated by the ratio between Pd and Pa [80/86 = 0.93], indicating that this left main lesion in itself was not significant from a functional point of view. (D) About 30 seconds after cessation of adenosine infusion the pressure gradient disappears and returns to baseline. In this patient bypass surgery was deferred and he underwent PTCA of the proximal left anterior descending stenosis only. FFR of the LAD was 0.63 before and 0.94 after PTCA.