
Figure 2 .
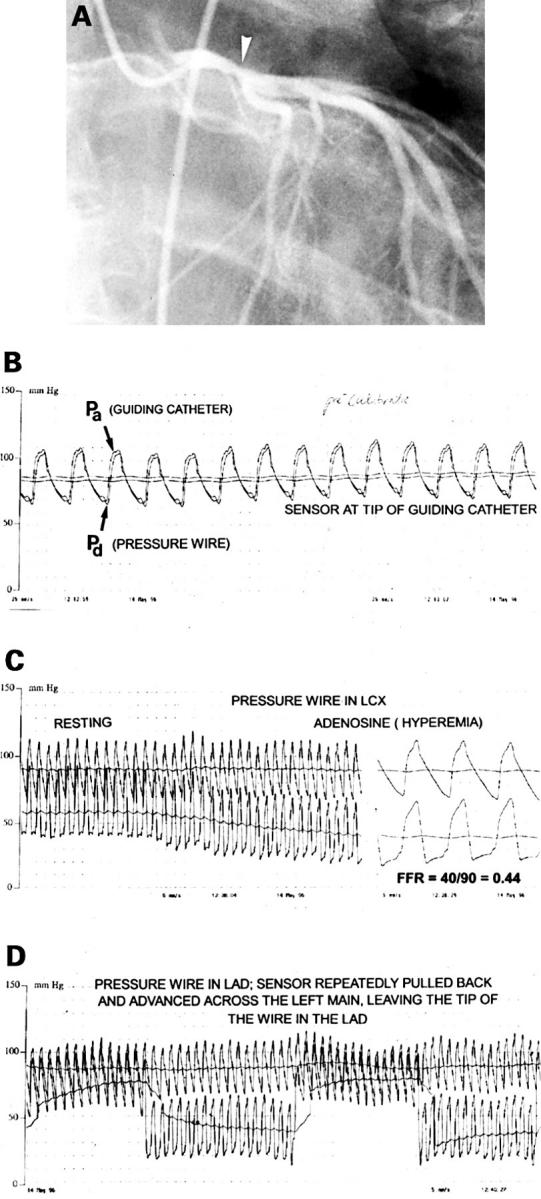
(A) Coronary angiogram in the right anterior oblique projection from a 36 year old man who experienced an anterior wall myocardial infarct, successfully treated by thrombolysis. At angiography only a 40% stenosis (arrow) of the distal left main coronary artery (LM) was visible, and there was mild hypokinesia of the anterior wall segments. Perfusion scintigraphy performed several weeks later was negative. The dilemma was whether to perform bypass surgery or to leave this lesion untreated. (B) A pressure wire is advanced to the tip of the coronary catheter, and equal pressures are registered at that position by the guiding catheter (Pa) and the pressure sensor (Pd ). (C) The pressure wire is advanced across the left main stenosis into the left circumflex coronary artery and a large gradient is observed at rest. After start of intravenous adenosine infusion (140 µg/kg/min), this gradient gradually further increases and at steady state maximum coronary hyperaemic myocardial fractional flow reserve is calculated by the ratio between Pd and Pa [40/90 = 0.44], indicating that this left main lesion is physiologically highly significant. (D) Shows how the wire is positioned in the left anterior descending coronary artery and slowly withdrawn and advanced across the left main stenosis. Because the pressure sensor is located at 3 cm from the tip of the wire, this pull-back/push-up procedure can be performed repeatedly under fluoroscopy. It confirms the presence and exact location of a stenosis. This patient was treated by bypass surgery.