

Abstract
Lead and mercury are naturally occurring elements in the earth's crust and are common environmental contaminants. Because people concerned about possible exposures to these elements often seek advice from their physicians, clinicians need to be aware of the signs and symptoms of lead and mercury poisoning, how to investigate a possible exposure and when intervention is necessary. We describe 3 cases of patients who presented to an occupational medicine specialist with concerns of heavy metal toxicity. We use these cases to illustrate some of the issues surrounding the investigation of possible lead and mercury exposures. We review the common sources of exposure, the signs and symptoms of lead and mercury poisoning and the appropriate use of chelation therapy. There is a need for a clear and consistent guide to help clinicians interpret laboratory investigations. We offer such a guide, with information about population norms, lead and mercury levels that suggest exposure beyond that seen in the general population and levels that warrant referral for advice about clinical management.
Exposure to environmental contaminants, including heavy metals, continues to be a widespread problem in Canada, and patients concerned about possible exposures often seek advice from their physicians. Heavy metals are a well-established cause of severe illness, and these concerns need to be addressed. However, although clinically significant exposures to heavy metals still occur in Canada, a substantial proportion of patients who present with concerns of heavy metal toxicity do not have true poisoning. Physicians need to be aware of not only the signs and symptoms of heavy metal poisoning but also what investigations are appropriate, how to interpret the results, when intervention is necessary and when it is unwarranted. Alternative health care providers are also investigating and treating heavy metal exposures; therefore, it is helpful to be familiar with the treatments they are offering and some of the pitfalls their patients may fall into.
In this review, we describe 3 cases of patients referred to an occupational medicine specialist with concerns of heavy metal toxicity. One was referred with symptoms of severe poisoning from an unknown source, the others with significant anxiety about possible occupational exposures and conflicting laboratory investigations. One patient had already consulted and had received treatment from an alternative health care provider. These cases have been chosen to illustrate some of the issues that commonly arise around concerns of exposure to heavy metals, in particular lead and mercury. We also provide a guide to interpreting laboratory investigations to assist clinicians with investigating concerns and advising their patients.
Cases
Case 1
A 54-year-old East Indian man consulted his family physician because of fatigue, abdominal pain, nausea, headaches and weight loss. Investigations ordered by the family physician included measurement of the hemoglobin concentration, which was 73 g/L. The pathologist who reviewed the laboratory test results commented on the low mean cell volume and coarse basophilic stippling of the red blood cells. The blood lead level was therefore measured and found to be markedly elevated, at 4.15 (reference range < 1.93) μmol/L. It was eventually determined that the patient had been taking traditional medicines imported from India for over 2 years. Analysis revealed that they contained 13%– 14% (130 000 μg/g) lead and 1% (10 000 μg/g) mercury by weight. The patient was referred to a clinical toxicologist and underwent chelation therapy, with substantial improvement of his symptoms and anemia. At follow-up several months after his last chelation treatment, his blood lead level was 1.34 μmol/L and hemoglobin concentration 129 g/L.
Case 2
A 35-year-old dentist presented with a 1-year history of a fine resting tremor in his hands. This is a serious occupational disability for him, because it interferes with his ability to perform the fine motor tasks required in dental practice. He was assessed by a neurologist, who diagnosed benign tremor. The patient became concerned about possible mercury toxicity because of some occupational exposure to mercury and asked his family physician to arrange for testing. Results from tests conducted at a laboratory in Quebec City revealed that his blood mercury level was 18 (reference range < 15) nmol/L, and his mercury level in a 24-hour urine collection was reported as “normal.” The patient began reducing his exposure to mercury amalgam and requested a consultation with an occupational medicine specialist to discuss chelation therapy. Repeat testing at a laboratory in Vancouver revealed a blood mercury level of 19 (reference range < 29) nmol/L and a mercury level in a 24-hour urine collection of 29 (reference range < 50) nmol/d. The patient was not reassured by these results, since he found the different reference ranges used by the 2 laboratories confusing.
Case 3
A 44-year-old woman worked for 10 months in a car dealership and service centre. In the course of her work, she was exposed to vehicle emissions and other substances present in the service area. There was no established exposure to heavy metals. The woman developed a variety of symptoms, including pain and tingling in one hand, abdominal pain and bloating, diarrhea and constipation, increased bruising, varicose veins and fatigue. After 10 months she left the car dealership. Her symptoms improved, but she remained concerned and consulted an alternative health care provider. He arranged testing for blood lead and blood mercury levels and a “24-hour urine toxic metals test,” which entailed challenging the patient with a chelating agent and subsequently measuring the levels of various heavy metals in her urine. Her blood lead level was 0.1 (reference range < 1.93) μmol/L and her blood mercury level 10 (reference range < 29) nmol/L. However, the results of the toxic metals test were presented in such a way as to suggest lead and mercury toxicity. The alternative health care provider diagnosed heavy metal poisoning from her working at the car dealership and started the patient on chelation therapy. The patient's family physician questioned this course of action and arranged for consultation with an occupational medicine specialist.
Lead
Lead is used in many industries, including lead smelting and processing, the manufacturing of batteries, pigments, solder, plastics, cable sheathing, ammunition and ceramics, and battery recycling.1 In the United States, most cases of lead poisoning in adults result from occupational exposure, although lead exposure in the general population is primarily through diet.2 Whether the same is true in Canada is uncertain, since population-based surveillance of exposure to lead or other environmental contaminants is not performed in this country. In addition to diet as a source of exposure, there is ongoing lead exposure in the general population from old lead-based paint.3 Average blood lead levels in the northeastern and midwestern United States are higher than those in the southern and western regions, in part because of the increased presence of lead in older homes.4,5 Heavy metals, including lead, are used in the manufacture of Ayurvedic medicinal products, and nonstandardized manufacturing may result in high levels remaining in the final product.6 A recent study of Ayurvedic medicinal products sold in the Boston area revealed that 20% contained heavy metals.7 These products are commonly imported from India, both for resale and for private use. Reductions in the use of lead in food processing, the removal of lead additives from gasoline and the reduction of lead in paint have resulted in marked declines in lead exposure in the North American population. Data from the United States show that the mean blood lead level in the US population decreased from 0.71 to 0.07 μmol/L (14.6 to 1.5 μg/dL) between 1976 and 2001/02.3,8
Inorganic and organic forms of lead are absorbed through the lungs and gastrointestinal tract; organic lead compounds may also be absorbed through the skin. In occupational settings, exposure through inhalation is more common, whereas in the general population it is largely through ingestion.9 Following absorption, lead is taken up in the blood and deposited in soft tissues (brain, liver, kidney, bone marrow) and bone. Excretion is primarily via the kidneys, and the half-life of lead in the blood is about 30 days. Up to 94% of the body burden of lead is in bone, where it has a half-life of years to decades.3,9 Pregnancy, lactation, menopause, osteoporosis and other events that lead to increased bone resorption will lead to an increase in blood lead levels in people who have substantial amounts of lead stored in bone, and it can be an unexpected source of lead poisoning.9
Signs and symptoms of lead poisoning in adults may include abdominal pain, anorexia, nausea and constipation, headache, joint and muscle pain, difficulties with concentration and memory, sleep disturbances, anemia with basophilic stippling, peripheral neuropathy and nephropathy.3,9
The blood lead level is the most widely used and most reliable measure of lead exposure. It primarily measures exposures that have taken place in the previous few weeks10 but is a poor indicator of lead accumulated in bone. Bone lead levels are theoretically the best indicator of total body burden; however, measurement is difficult. X-ray fluorescence can be used to monitor lead in the skeleton, but the technique is not widely available and is generally used only for research.11 Contamination of blood and urine specimens during collection and storage is a potential problem when screening for heavy metals, and adherence to strict guidelines from a reputable laboratory is important. The use of metal-free collection devices and storage tubes is essential.
Interpretating blood lead levels requires an understanding of reference ranges and how they are derived. Although lead is toxic and serves no biological purpose, it is a naturally occurring element, and some degree of exposure is universal. Reference ranges may vary from laboratory to laboratory; in some cases they are based on levels commonly or normally seen in a particular population, and in others they are derived from exposure limits (e.g., benchmark doses) published by national or international agencies.12 Although symptoms in adults generally do not appear until blood lead levels reach at least 1.9 μmol/L (40 μg/dL), adverse effects from lead exposure in adults can be measured at levels as low as 0.5 μmol/L (10 μg/dL), and a definitive threshold below which no adverse effects will occur has not yet been established.3,9,13 Children and fetuses are more susceptible and may show lasting effects from blood lead concentrations below 0.5 μmol/L (10 μg/dL).14,15 Case 1 highlights the fact that heavy metal poisoning does occur in Canada and that physicians need to consider the possibility in their differential diagnoses.
Mercury
Mercury exists in elemental (metallic), inorganic and organic (methylated) forms. The general population is primarily exposed to mercury vapour from dental amalgam and to organic mercury from fish consumption. Mercury bioaccumulates up the food chain; therefore, large predatory species such as tuna, shark and swordfish may have high concentrations of mercury in their tissue.16–18 Occupational exposure to mercury is generally to mercury vapour and can occur in dentistry, mining, and the manufacture of electrical equipment and medical instruments.19 Thimerosal, a mercury-containing preservative, is a component of some vaccines but has been phased out from most routine childhood vaccinations.20 Mercury can also be found in Ayurvedic medicinal products.6,7
The route of exposure and efficiency of absorption depends on the form of mercury. Mercury vapour is well absorbed through the respiratory route, but absorption of elemental mercury is negligible through the oral route. Oral absorption of inorganic mercury compounds is poor to moderate depending on the precise form. Oral absorption of organic mercury is nearly complete. Once absorbed, mercury is distributed primarily to the central nervous system and the kidneys. Elimination is through the urine and feces. The half-life of elemental and inorganic mercury in the blood is 40–60 days, and the half-life of organic mercury in the blood is about 70 days.3,16,17
Signs and symptoms of mercury toxicity vary with the form of mercury and route of exposure but include gingivitis, stomatitis and excessive salivation. Sensory peripheral neuropathy is common, and central nervous system effects include personality changes, irritability, fatigue, tremor (usually intention tremor), ataxia, difficulties with memory and concentration, sleep disturbances and a metallic taste. Renal effects include both tubular and glomerular damage. In the fetus, organic mercury disrupts the cytoarchitecture of the developing brain and has been associated with neuropsychological changes after birth.3,16,17
Mercury levels can be measured in both blood and urine. Either form of measurement can be used to assess exposures to elemental and inorganic forms of mercury, although individuals with a past history of exposure may have elevated urine levels without elevated blood levels. Measurement of mercury in whole blood is the preferred test for exposure to organic mercury, since this form of mercury is excreted primarily in the feces rather than in the urine.3,16,21 It is important to choose the appropriate test depending on the suspected source of exposure.
As with lead, interpreting mercury levels requires some understanding of the reference ranges. Mercury is naturally present in the earth's crust, and some degree of exposure is inevitable. Reference ranges for mercury may be based on values commonly seen in a particular population or they may be derived from benchmark doses. Data taken from communities inadvertently exposed to mercury and from populations that consume large quantities of seafood suggest that adverse effects in the most vulnerable subpopulation — developing fetuses — may start at steady state maternal blood levels as low as 200 nmol/L (40 μg/L).22–24 In adults, clinically observable signs of tremor, ataxia and paresthesias begin to occur at blood levels of about 500 nmol/L (100 μg/L).3,16 Case 2 illustrates some of the difficulties inherent in interpreting test results. The dentist's initial blood mercury level (18 nmol/L) was measured at a laboratory whose reference range (< 15 nmol/L) reflects the norms seen in the population of the Quebec City area. The second measurement (19 nmol/L) was measured at a Vancouver laboratory whose reference range (< 29 nmol/L) is set as a percentage of the US Environmental Protection Agency's benchmark dose for mercury (290 nmol/L). Neither the patient nor the ordering physician knew what to make of the results, and in the absence of an understanding of how to interpret the reference ranges, the patient became concerned that he was experiencing mercury poisoning. It required several additional encounters to persuade the patient that this was not the case.
Guide to interpreting laboratory results
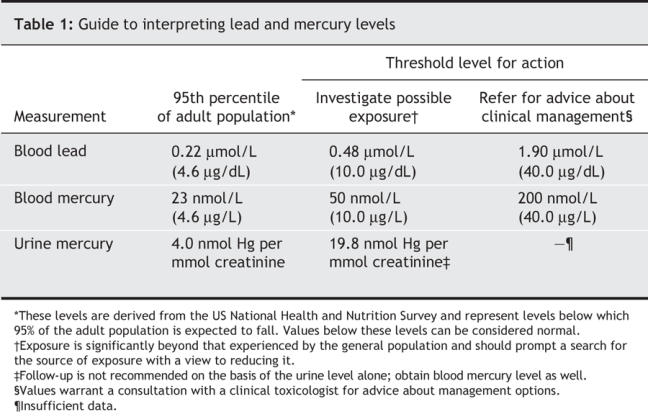
There is a need for a clear and consistent guide to assist clinicians in interpretating laboratory test results of lead and mercury levels. Such a guide should provide information on population norms, levels that suggest exposure beyond that seen in the general population and levels that warrant consultation for advice about clinical management. Based on a review of the lead and mercury toxicology literature, available population-based surveys of exposure and experience in clinical follow-up of patients with a history of exposure, we propose the guide presented in Table 1.3,13,25
Table 1
Interventions
The first step in treating all cases of heavy metal toxicity is to reduce or remove the source of exposure. In most cases this is all that is required.3,16 Chelation therapy has historically been used to reduce the body burden of heavy metals in patients with severe symptoms and highly elevated circulating levels of heavy metals.26 It is a process in which heavy metals are removed from the body with the use of a chelating agent, a charged molecule that binds metals in a stable complex known as a chelate. The chelate is subsequently excreted in the urine.27 The decision as to which patients should receive chelation therapy is a matter of clinical judgment. Although the ability of chelating agents to bind heavy metals and increase elimination of those metals in the urine is well established, our review of the Cochrane database revealed a significant shortage of controlled clinical trials that have evaluated the benefits of chelation therapy in reducing symptoms or in preventing long-term effects in adults with heavy metal poisoning. However, there is evidence that some patients given a course of chelation therapy may experience a placebo effect.28 There are no specific blood or urine levels above which treatment with a chelating agent is always indicated. The decision to proceed requires expert advice and is based on the duration of exposure, the patient's symptoms and the laboratory test results. Chelation therapy should be carried out only in a hospital setting by experienced physicians.2,19 Case 1 is an example of a symptomatic patient with a high body burden of lead who had substantial relief of symptoms from chelation therapy carried about by an experienced clinical toxicologist.
The “24-hour urine toxic metals test” that the patient in case 3 underwent deserves further comment. This procedure is more commonly known as the chelation challenge test or provocation chelation. It entails measuring urine levels of heavy metals before and after a single loading dose of a known chelating agent. It has been used to determine whether chelation therapy is indicated but is also used by some alternative health care providers to diagnose heavy metal poisoning. There is no good evidence supporting the use of the chelation challenge test for either purpose, and findings from some studies have suggested that it can lead to misleading diagnostic advice.29,30 Reference ranges for blood and urine levels intended for the general population cannot be meaningfully applied to people undergoing this test. In addition, there have been reports of serious and fatal reactions to the chelating agent, and findings from animal studies have suggested that a single dose of a chelating agent will merely mobilize heavy metals, which will then redistribute to more vulnerable tissues such as the central nervous system.29,31–33
Case 3 illustrates how the chelation challenge test can be misused. The patient's blood lead and blood mercury levels were normal. However, following the chelation challenge test, analysis of her urine did show the presence of heavy metals (a normal response to the chelating agent). Her urine levels were compared with those of “a normal population under nonchallenge conditions” (people who had not been administered a chelating agent), and on the basis of this invalid comparison, the alternative health care provider diagnosed lead and mercury poisoning and the patient agreed to a course of outpatient chelation therapy. Once the patient was offered an explanation as to how the result of the chelation challenge test had been misinterpreted, she discontinued the therapy. There is no good evidence of benefits from chelation therapy in cases in which the patient is asymptomatic or mildly symptomatic and has blood and urine levels comparable to population norms. It is not only unnecessary and costly, but it also places the patient at risk of a reaction to the chelating agent and may bind other positively charged minerals necessary for normal physiologic function.26,31
Heavy metal poisoning is a small but important public health problem in Canada. Patients who present with concerns of exposure require appropriate investigation. Many will not have true toxicity, but unless they are offered clear and comprehensive information, they may seek treatment elsewhere and risk being given misleading advice and potentially dangerous treatment. For patients who have elevated blood or urine levels of heavy metals, the problem can usually be managed by simply reducing or removing the source of exposure. Referral to the local public health unit can assist in identifying the source of an atypical exposure and may lead to additional case finding and removal of a source of exposure to the population. A decision to proceed to chelation therapy should be made only in consultation with an expert.
Footnotes
This article has been peer reviewed.
Contributors: Elizabeth Brodkin participated in the conception and design of the article, drafted the manuscript and was a member of the team that interviewed and worked up the 3 patients referred to in the article. Ray Copes participated in the conception and design of the article. Andre Mattman was responsible for the analysis and interpretation of the laboratory data. James Kennedy was responsible for the interpretation of the clinical data and treated one of the patients referred to in the article. Rakel Kling conducted a substantial portion of the literature review and was a member of the team that interviewed and worked up the 3 patients referred to in the article. Annalee Yassi participated in the conception and design of the article and led the team that interviewed and worked up the 3 patients referred to in the article. All of the authors revised the manuscript for critical content and approved the final version to be published.
Competing interests: None declared.
Correspondence to: Dr. Elizabeth Brodkin, Community Medicine Residency Program, Department of Health Care and Epidemiology, Faculty of Medicine, University of British Columbia, 5804 Fairview Ave., Vancouver BC V6T 1Z3; ebrodkin@interchange.ubc.ca
REFERENCES
- 1.Fischbein A. Occupational and environmental exposure to lead. In: Rom WN, editor. Environmental and occupational medicine. 3rd ed. Philadelphia: Lippincott-Raven; 1998. p. 973-96.
- 2.Adult blood lead epidemiology and surveillance — United States, 2002. MMWR Morb Mortal Wkly Rep 2004;53:578-82. [PubMed]
- 3.US Centers for Disease Control and Prevention (CDC). Third national report on human exposure to environmental chemicals. Atlanta: CDC; 2005. Available: www.cdc.gov/exposurereport/3rd/default.htm (accessed 2006 Oct 11).
- 4.Meyer PA, Pivetz T, Dignam TA; US Centers for Disease Control and Prevention. Surveillance for elevated blood lead levels among children — United States, 1997–2001. MMWR Surveill Summ 2003;52:1-21. [PubMed]
- 5.Jacobs DE, Clickner RP, Zhou JY, et al. The prevalence of lead-based paint hazards in US housing. Environ Health Perspect 2002;110:A599-606. [DOI] [PMC free article] [PubMed]
- 6.Health Canada warns consumers not to use certain Ayurvedic medicinal products. Ottawa: Health Canada; 2005 July 14. Available: www.hc-sc.gc.ca/ahc-asc/media/advisories-avis/2005/2005_80_e.html (accessed 2006 Oct 11).
- 7.Saper RB, Kales SN, Paquin J, et al. Heavy metal content of Ayurvedic herbal medicine products. JAMA 2004;292:2868-73. [DOI] [PubMed]
- 8.Annest JL, Mahaffey KR; National Center for Health Statistics. Blood lead levels for persons ages 6 months– 74 years: United States 1976–80 [Vital and Health Statistics series 11, no 233]. DHHS Pub no (PHS) 84-1683. Washington (DC): Public Health Service, US Department of Health and Human Services; 1984. Available: www.cdc.gov/nchs/data/series/sr_11/sr11_233.pdf (accessed 2006 Oct 11).
- 9.Agency for Toxic Substances and Disease Registry (ATSDR). Toxicological profile for lead [draft]. Washington (DC): ATSDR, Public Health Service, US Department of Health and Human Services; 2005. Available: www.atsdr.cdc.gov/toxprofiles/tp13.html (accessed 2006 Oct 11).
- 10.Graziano JH. Validity of lead exposure markers in diagnosis and surveillance. Clin Chem 1994;40:1387-90. [PubMed]
- 11.Hu H. Bone lead as a new biologic marker of lead dose: recent findings and implications for public health. Environ Health Perspect 1998;106(S4):961-7. [DOI] [PMC free article] [PubMed]
- 12.Faustman EM, Omenn GS. Risk assessment. In: Klaassen CD, editor. Casarett and Doull's toxicology: the basic science of poisons. 6th ed. New York: McGraw-Hill; 2001. p. 83-104.
- 13.US Environmental Protection Agency (EPA). Lead and compounds (inorganic) [CASRN 7439-92-1]. Washington (DC): Integrated Risk Information System, EPA; 2004. Available: www.epa.gov/iris/subst/0277.htm (accessed 2006 Oct 11).
- 14.Canfield RL, Henderson CR, Cory-Slechta DA, et al. Intellectual impairment in children with blood lead concentrations below 10 μg per deciliter. N Engl J Med 2003;348:1517-26. [DOI] [PMC free article] [PubMed]
- 15.Lanphear BP, Hornung R, Khoury J, et al. Low-level environmental lead exposure and children's intellectual function: an international pooled analysis. Environ Health Perspect 2005;113:894-9. [DOI] [PMC free article] [PubMed]
- 16.Agency for Toxic Substances and Disease Registry (ATSDR). Toxological profile for mercury. Washington (DC): ATSDR, Public Health Service, US Department of Health and Human Services; 1999. Available: www.atsdr.cdc.gov/toxprofiles/tp46.html (accessed 2006 Oct 11).
- 17.Clarkson TW, Magos L, Myers GJ. The toxicology of mercury — current exposures and clinical manifestations. N Engl J Med 2003;349:1731-7. [DOI] [PubMed]
- 18.US Department of Health and Human Services (DHHS) and US Environmental Protection Agency (EPA). Mercury levels in commercial fish and shellfish. Washington (DC): DHHS and EPA; 2001. Available: www.cfsan.fda.gov/~frf/sea-mehg.html (updated Feb 2006; accessed 2006 Oct 11).
- 19.Evans HL. Mercury. In: Rom WN, editor. Environmental and occupational medicine. 3rd ed. Philadelphia: Lippincott-Raven; 1998. p. 997-1003.
- 20.Bigham M, Copes R. Thiomersal in vaccines: balancing the risk of adverse effects with the risk of vaccine-preventable disease. Drug Saf 2005;28:89-101. [DOI] [PubMed]
- 21.Baselt RC. Biological monitoring methods for industrial chemicals. 2nd ed. Littleton (MA): PSG Publishing Co.; 1988.
- 22.US Environmental Protection Agency (EPA). Methylmercury (MeHg) [CASRN 22967-92-6]. Washington (DC): Integrated Risk Information System, EPA; 2001. Available: www.epa.gov/IRIS/subst/0073.htm (accessed 2006 Oct 11).
- 23.US Environmental Protection Agency (EPA). Fish tissue criterion for methylmercury to protect human health document. Washington (DC): EPA; 2000. Available: www.epa.gov/waterscience/criteria/methylmercury/document.html (accessed 2006 Nov 17).
- 24.Bureau of Chemical Safety, Food Directorate. Review of the tolerable daily intake for methylmercury. Ottawa: Health Protection Branch, Health Canada; 1998 Apr 27. [internal memo]
- 25.American Conference of Governmental Industrial Hygienists. Mercury, elemental and inorganic: BEI. 7th ed. Documentation. Cincinnati: ACGIH; 2001.
- 26.Risher JF, Amler SN. Mercury exposure: evaluation and intervention, the inappropriate use of chelating agents in the diagnosis and treatment of putative mercury poisoning. Neurotoxicology 2005;26:691-9. [DOI] [PubMed]
- 27.Kalia K, Flora SJS. Strategies for safe and effective therapeutic measures for chronic arsenic and lead poisoning. J Occup Health 2005;47:1-21. [DOI] [PubMed]
- 28.Grandjean P, Guldager B, Larsen IB, et al. Placebo response in environmental disease: chelation therapy of patients with symptoms attributed to amalgam fillings. J Occup Environ Med 1997;39:707-14. [DOI] [PubMed]
- 29.Archbold GP, McGuckin RM, Campbell NA. Dimercaptosuccinic acid loading test for assessing mercury burden in healthy individuals. Ann Clin Biochem 2004;41:233-6. [DOI] [PubMed]
- 30.Frumkin H, Manning CC, Williams PL, et al. Diagnostic chelation challenge with DMSA: A biomarker of long-term mercury exposure? Environ Health Perspect 2001;109:167-71. [DOI] [PMC free article] [PubMed]
- 31.Deaths associated with hypocalcemia from chelation therapy — Texas, Pennsylvania and Oregon, 2003–2005. MMWR Morb Mortal Wkly Rep 2006;55:204-7. [PubMed]
- 32.Ewan KB, Pamphlett R. Increased inorganic mercury in spinal motor neurons following chelating agents. Neurotoxicology 1996;17:343-9. [PubMed]
- 33.Cory-Slechta DA, Weiss B, Cox C. Mobilization and redistribution of lead over the course of calcium disodium ethylenediamine tetraacetate chelation therapy. J Pharmacol Exp Ther 1987;243:804-13. [PubMed]