
Figure 6 .
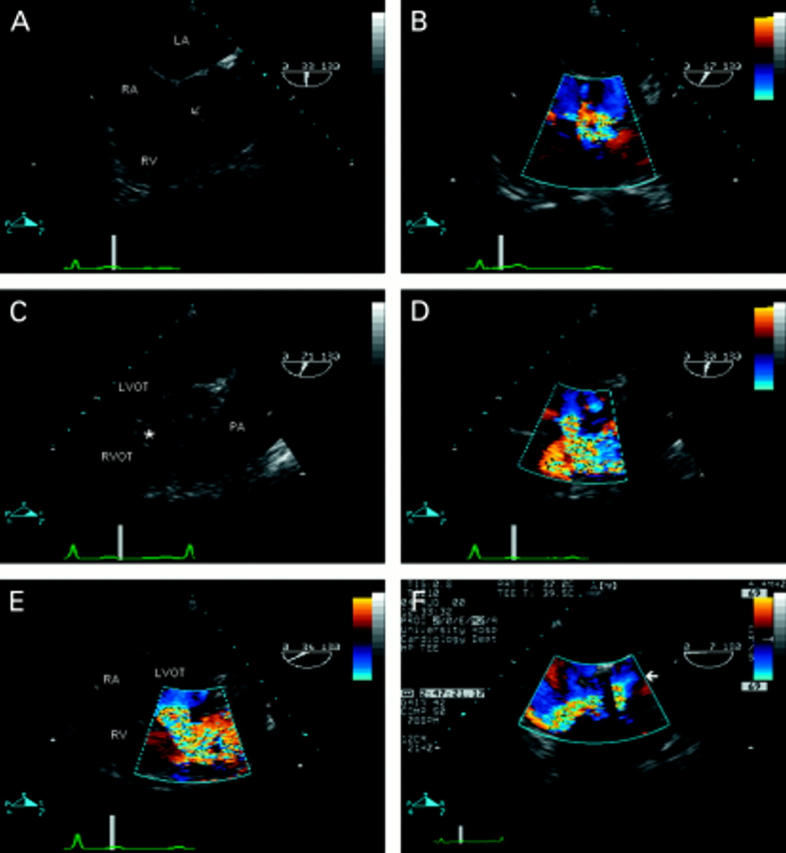
Ventricular septal defect (VSD) seen in the transverse plane of the left ventricular outflow tract (A). There is a defect in the perimembraneous region (arrow), partially plugged by tricuspid valve tissue. Colour flow mapping (B) reveals the presence of a left-to-right shunt—note the flow convergence zone in the left ventricular outflow tract—confirming the diagnosis of perimembraneous VSD. (C) Oblique view showing the right ventricular outflow tract in its long axis, in a patient with aortic valve endocarditis—note the vegetation seen in the left ventricular outflow tract. There is a defect seen between the two outflow tracts (*). The right ventricular infundibulum is hypertrophied, resulting in the appearance of subpulmonary stenosis, and the pulmonary artery is dilated. The diagnosis of doubly committed VSD is confirmed by colour flow mapping (D). (E) The same defect in the short axis view. Note that the defect is between left ventricular outflow tract and right ventricular outlet rather than between left ventricular outflow tract and right ventricular inlet as with perimembraneous defects (B). The importance of the flow convergence zone is demonstrated in F. The four chamber view with flexion reveals the left ventricular outflow tract in a patient with two previous aortic valve replacements. An apparent jet of tricuspid regurgitation is seen in the right atrium. However, note that this flow originates from the left ventricular outflow tract (arrow)—that is, there is a communication between the left and right ventricle. The dropout within the colour map is caused by artefact from the aortic valve replacement. RA, right atrium; RV, right ventricle; LV, left ventricle; RVOT, right ventricular outflow tract; LVOT, left ventricular outflow tract; LA, left atrium; PA, pulmonary artery.