

A 61 year old man, undergoing dialysis because of chronic renal failure, was admitted for examination with high grade fever. A blood sample was positive for methicillin resistant Staphylococcus aureus. During his stay in hospital, he complained of acute chest pain associated with ST elevation in leads II, III, aVF. Transthoracic echocardiography (TTE) showed an akinetic inferior wall and a smooth bulging mass located along the atrioventricular groove (panel A). Colour Doppler imaging revealed blood flow from the bulging mass into the right atrium (panel B). No vegetations were noted on TTE. Coronary angiography demonstrated a large aneurysm of the right coronary artery, which was occluded by thrombus (panel C). Contrast media injected into the right coronary artery drained to the right atrium (panel D). The patient underwent resection of the aneurysm and patch closure of the perforation following removal of the aneurysm. Histological examination showed it was a mycotic aneurysm.
The patient’s postoperative course was uneventful, and he was discharged from hospital and placed on a long course of antibiotics.
Coronary artery mycotic aneurysms are often silent until either thrombosis results in myocardial infarction or the aneurysm ruptures producing massive haemopericardium and cardiac tamponade. Given the rarity of the condition, an extremely high index of clinical suspicion is necessary for the diagnosis.
Figure 1.

Figure 2.
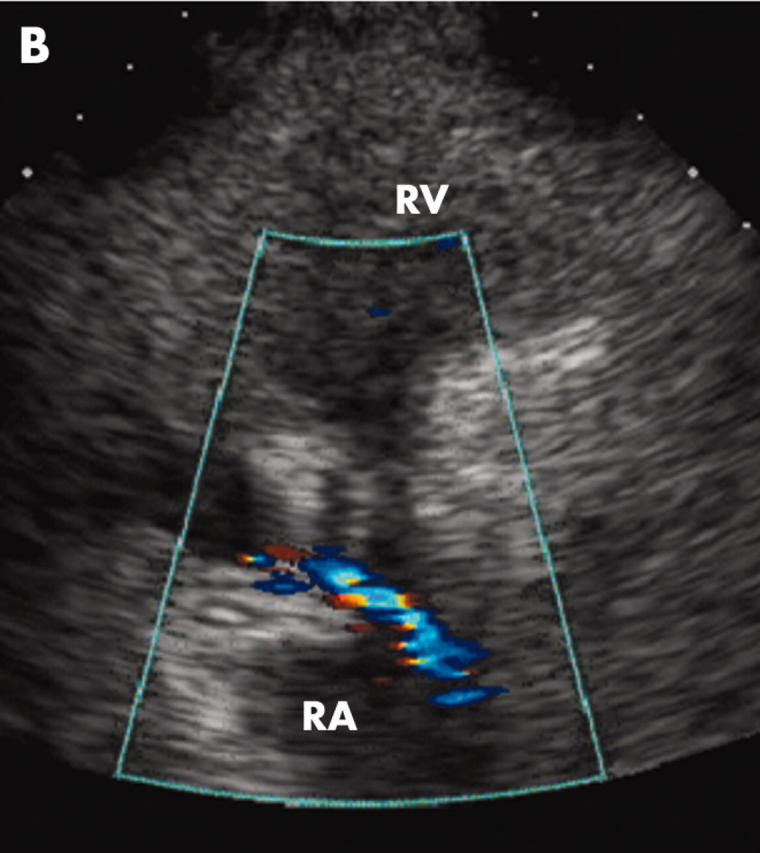
Figure 3.

Figure 4.
