
Figure 3.
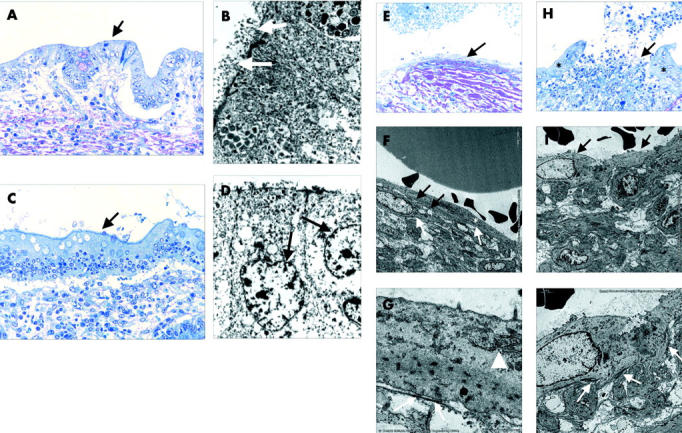
Electron micrographs of epithelialised and non-epithelialised fistulae of Crohn’s disease patients and controls. (A–D) Re-epithelialised fistulae of the small intestine (A: semithin section, toluidine blue, ×200; B: electron micrograph) and colon (C: semithin section, toluidine blue, ×200; D: electron micrograph). Histomorphologically, there is no similarity to the original lining epithelium of the small intestine (A: arrow) or colon (C: arrow) but by electron micrography there are typical microvilli (B: white arrows) and goblet cells (D: arrows). (E–G) Central fissure of a fistula lined by myofibroblasts (E: arrow). There is the typical appearance of myofibroblasts (F: asterisks): a cell membrane with multiple caveolae (F: white arrows), a rough endoplasmic reticulum and Golgi complex, and the cytoplasm containing bundles of microfilaments with focal densities (G: arrowhead). Myofibroblasts are connected to each other by adherens and gap junctions (F: black arrows) and are in contact with a newly formed thin basement membrane by fibronexus (G: white arrows). (H–J) Central fissure of a fistula lined by epithelium (H: asterisks) and myofibroblasts (H: arrow). The myofibroblasts rest irregularly on the surface of the fissure of the fistula (I: arrows), there are no generated adherens or gap junctions, and the underlining newly formed basement membrane (J: white arrows) is not continuous.