
Figure 3.
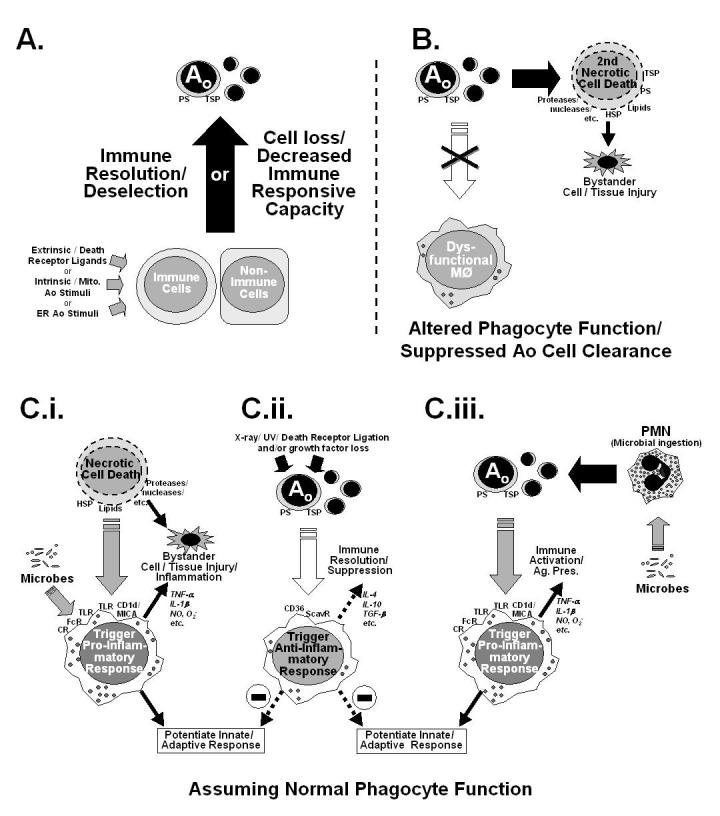
A depiction of several possible mechanisms of immune suppression. (A) Illustrates the simple hypothesis (mechanism) that the immune dysfunction observed is a result of advertant/inadvertent apoptotic (Ao) loss of immune cell potential/capacity resultant from extrinsic and/or intrinsic Ao pathway activation. Here no consideration is made for Ao cell clearance. (B) Depicts a scheme in which phagocytic function is compromised, so as to block apoptotic cell clearance, subsequently allowing apoptotic cells to move into secondary necrosis, that may in turn produce by-stander tissue injury. The scenarios illustrated in C.i.-C.iii. represent the proposed effects that clearance of necrotic (C.i.) and/or apoptotic cell materials (induced by classic Ao stimuli [C.ii.] or ingestion of microbes [C.iii.])has on the developing macrophage functional phenotype (pro-inflammatory vs. anti-inflammatory/immune suppressive) is considered when phagocytic function is normal. CD36, cell differentiation antigen 36; CR, complement receptor(s); CD1d/MICA non-variant major histocompatability class 1-like antigen family; FcR, immunoglobulin constant region receptor(s); HSP, heat shock protein(s); PS, phosphotydal serine; ScavR, Scavenger receptor(s) which bind PS; TSP, thrombospondin.