
Figure 3.
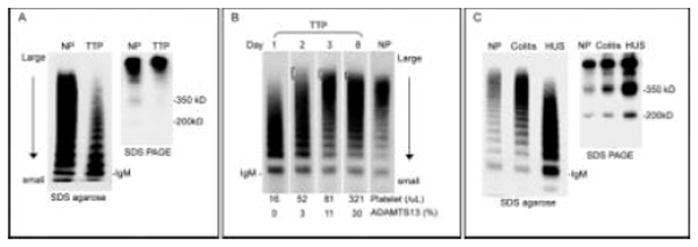
VWF multimer changes in TTP and HUS. A. VWF multimers and fragments in a representative case of acute TTP. Compared to normal plasma (NP), a gradient of decreased large multimers is noted in TTP. The decrease of large multimers is due to consumption as shear stress induces binding of large VWF multimers to platelets. In the absence of ADAMTS13, the 350kD and 200kD fragments of VWF are decreased. B. Serial changes of VWF multimers in TTP. A typical loss of large multimers is noted on day 1. As the patient improves with plasma exchange, ultra large multimers are present in subsequent days. The multimer pattern shows a gradually shift toward normal as the platelet count and ADAMTS13 activity level increase (bottom). C. VWF multimers and fragments in a representative case of shiga toxin associated HUS. VWF multimer is normal during the stage of colitis but shows a gradient of decreased large multimers at the onset of HUS. The VWF fragments are markedly increased, which are attributable to both increased VWF antigen level and increased proteolysis by ADAMTS13 [74]. VWF multimers are separated by SDS agarose gel electrophoresis and visualized. VWF fragments are separated by SDS agarose PAGE under non-reducing conditions. VWF is visualized with rabbit polyclonal anti-VWF and 125I labeled or horseradish peroxidase labeled goat anti-rabbit IgG.