
Figure 2.
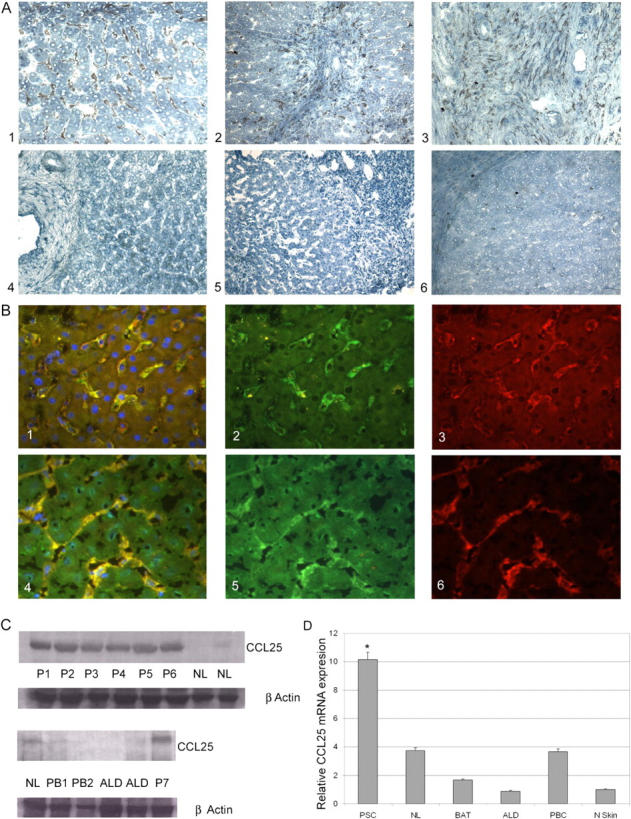
CCL25 expression in the liver. (A) The livers of patients with PSC demonstrated strong sinusoidal staining with CCL25 ab (A1, brown pigment), staining was particularly intense in periportal areas in association with areas of interface hepatitis (A2), and in portal tracts where macrophages/dendritic cells (confirmed by CD68 coexpression; not depicted) stained strongly (A3). There was no detectable CCL25 staining of hepatocytes, bile ducts, or vascular endothelium in normal liver (A4) or other chronic inflammatory diseases including primary biliary cirrhosis (A5). Staining with isotype-matched control antibodies was negative (A6). (B) Dual color immunofluorescence (B1/B4, yellow merged image) colocalized staining with CCL25 antibody (B2/B5, green) and CD31 antibody (B3, red) or LYVE-1 antibody (B6, red) to sinusoidal endothelial cells. Nulcei were counterstained with DAPI blue. (C) Western blotting confirmed the immunohistochemistry findings with detection of CCL25 in all PSC livers, but minimal detection in normal or other chronically inflamed livers. P1-7, PSC; NL, normal liver; PB1,2, PBC; ALD, alcoholic liver disease. Protein loading was normalized with β-actin staining. (D) Real-time PCR confirmed a 10-fold increase of CCL25 mRNA in PSC compared with control tissue (normal skin). *, P < 0.001. Modest amounts of CCL25 mRNA were detected in NL and other liver samples (BAT, biliary atresia; ALD and PBC) but the levels were not statistically significant compared with skin.