

Abstract
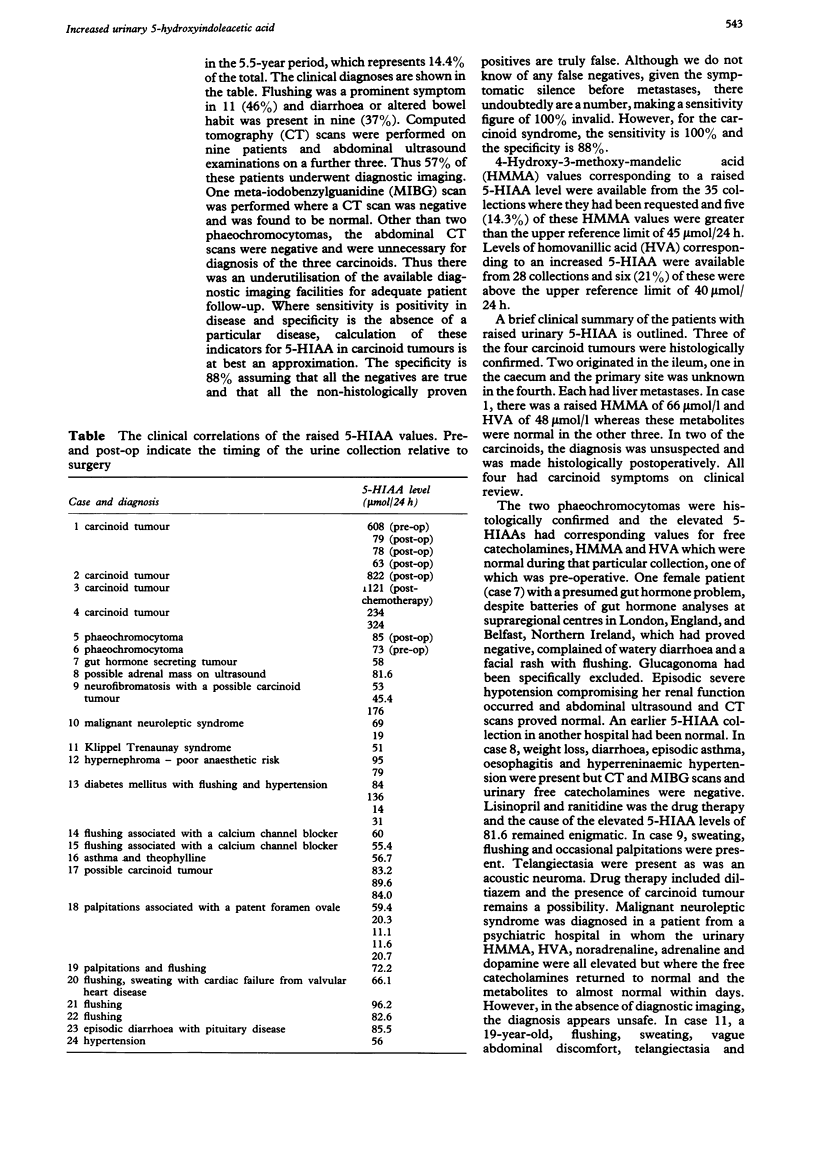
Over a five-and-a-half-year period, there were 298 laboratory requests for urinary 5-hydroxyindoleacetic acid (5-HIAA). The clinical and laboratory associations of the 24 patients in which there were 43 urinary 5-HIAA 24-h collection results greater than the laboratory upper reference limit are detailed. Four were confirmed carcinoid tumours and two were phaeochromocytomas. Flushing was a prominent symptom in 46% and diarrhoea or altered bowel habit in 37%. Associated with the raised urinary 5-HIAA values were increased levels of 4-hydroxy-3-methoxymandelic acid and homovanillic acid in 14.3% and 21%, respectively, of those collections where the metabolites were requested. Diagnostic imaging was performed in 57%. While the specificity was 88%, 5-HIAA is relatively insensitive in the diagnosis of carcinoid tumours and a more widespread use of diagnostic imaging including isotope scanning with labelled metaiodo-benzylguanidine, vasoactive intestinal peptide and octreotide is suggested.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Berge T., Linell F. Carcinoid tumours. Frequency in a defined population during a 12-year period. Acta Pathol Microbiol Scand A. 1976 Jul;84(4):322–330. [PubMed] [Google Scholar]
- Davidson D. F. Simultaneous assay for urinary 4-hydroxy-3-methoxy-mandelic acid, 5-hydroxyindoleacetic acid and homovanillic acid by isocratic HPLC with electrochemical detection. Ann Clin Biochem. 1989 Mar;26(Pt 2):137–143. doi: 10.1177/000456328902600208. [DOI] [PubMed] [Google Scholar]
- Deacon A. C. The measurement of 5-hydroxyindoleacetic acid in urine. Ann Clin Biochem. 1994 May;31(Pt 3):215–232. doi: 10.1177/000456329403100302. [DOI] [PubMed] [Google Scholar]
- Feldman J. M. Increased dopamine production in patients with carcinoid tumors. Metabolism. 1985 Mar;34(3):255–260. doi: 10.1016/0026-0495(85)90009-5. [DOI] [PubMed] [Google Scholar]
- Feldman J. M. Urinary serotonin in the diagnosis of carcinoid tumors. Clin Chem. 1986 May;32(5):840–844. [PubMed] [Google Scholar]
- Griffiths D. F., Williams G. T., Williams E. D. Multiple endocrine neoplasia associated with von Recklinghausen's disease. Br Med J (Clin Res Ed) 1983 Nov 5;287(6402):1341–1343. doi: 10.1136/bmj.287.6402.1341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hoefnagel C. A. Metaiodobenzylguanidine and somatostatin in oncology: role in the management of neural crest tumours. Eur J Nucl Med. 1994 Jun;21(6):561–581. doi: 10.1007/BF00173045. [DOI] [PubMed] [Google Scholar]
- Norheim I., Theodorsson-Norheim E., Brodin E., Oberg K. Tachykinins in carcinoid tumors: their use as a tumor marker and possible role in the carcinoid flush. J Clin Endocrinol Metab. 1986 Sep;63(3):605–612. doi: 10.1210/jcem-63-3-605. [DOI] [PubMed] [Google Scholar]
- Roberts L. J., 2nd, Marney S. R., Jr, Oates J. A. Blockade of the flush associated with metastatic gastric carcinoid by combined histamine H1 and H2 receptor antagonists. Evidence for an important role of H2 receptors in human vasculature. N Engl J Med. 1979 Feb 1;300(5):236–238. doi: 10.1056/NEJM197902013000506. [DOI] [PubMed] [Google Scholar]
- Watson R. G., Johnston C. F., O'Hare M. M., Anderson J. R., Wilson B. G., Collins J. S., Sloan J. M., Buchanan K. D. The frequency of gastrointestinal endocrine tumours in a well-defined population--Northern Ireland 1970-1985. Q J Med. 1989 Jul;72(267):647–657. [PubMed] [Google Scholar]