

Abstract
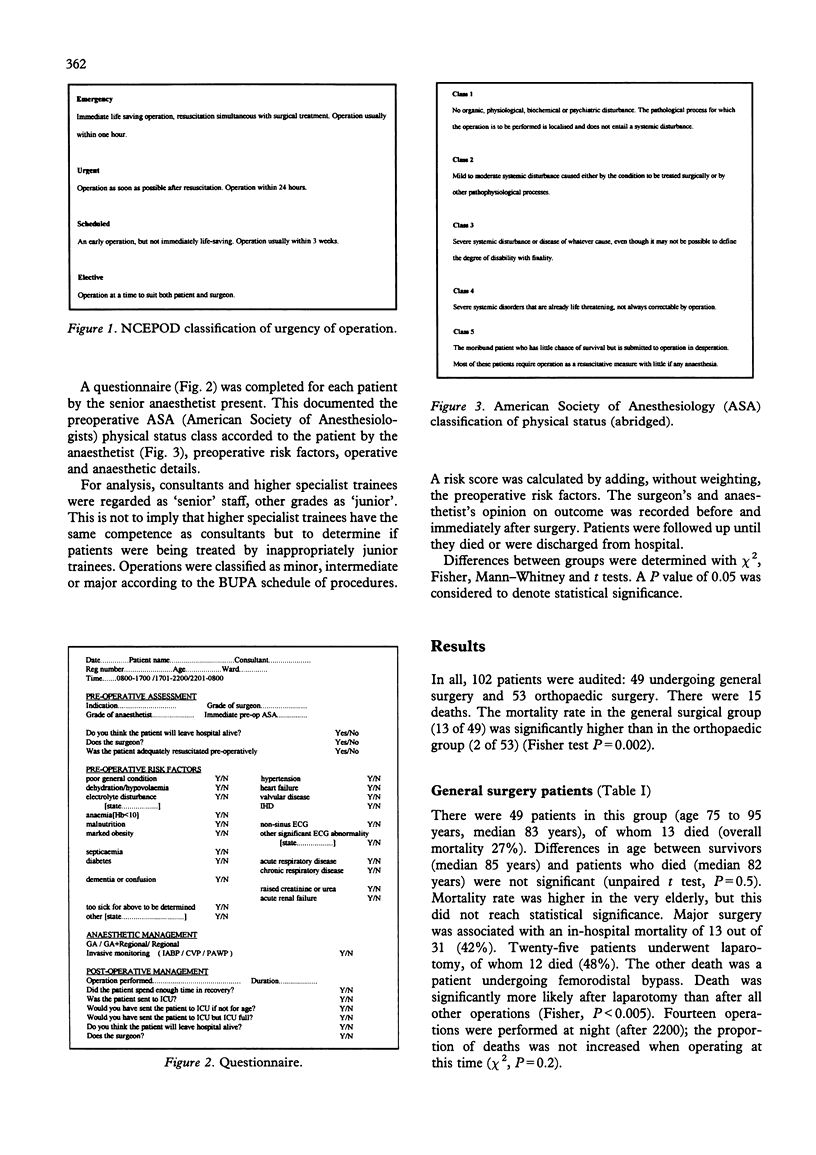
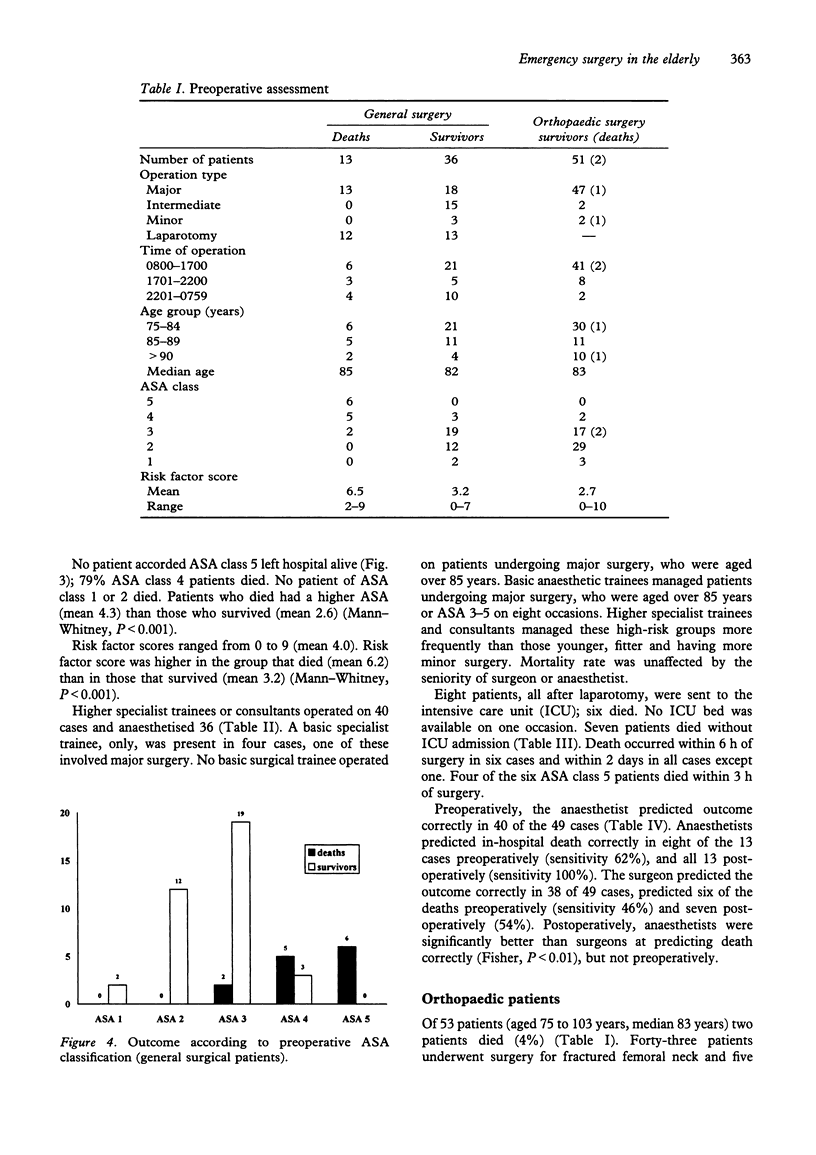
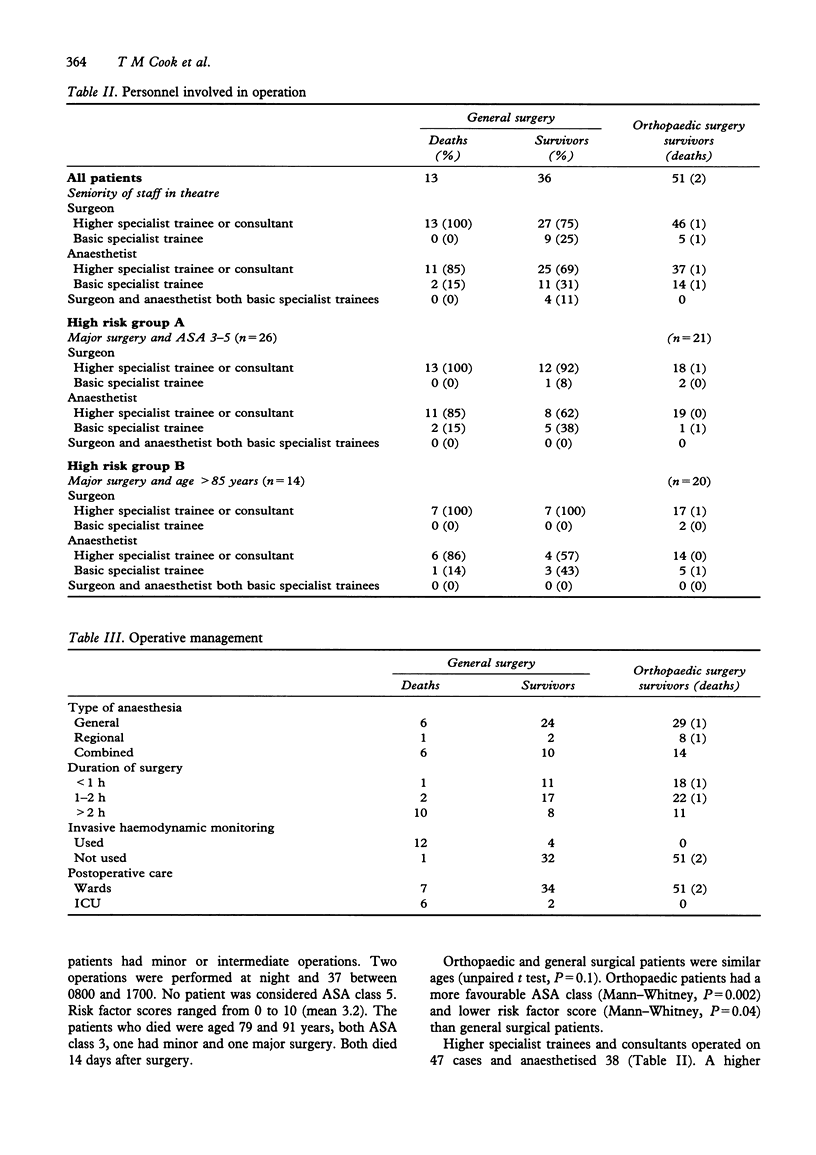
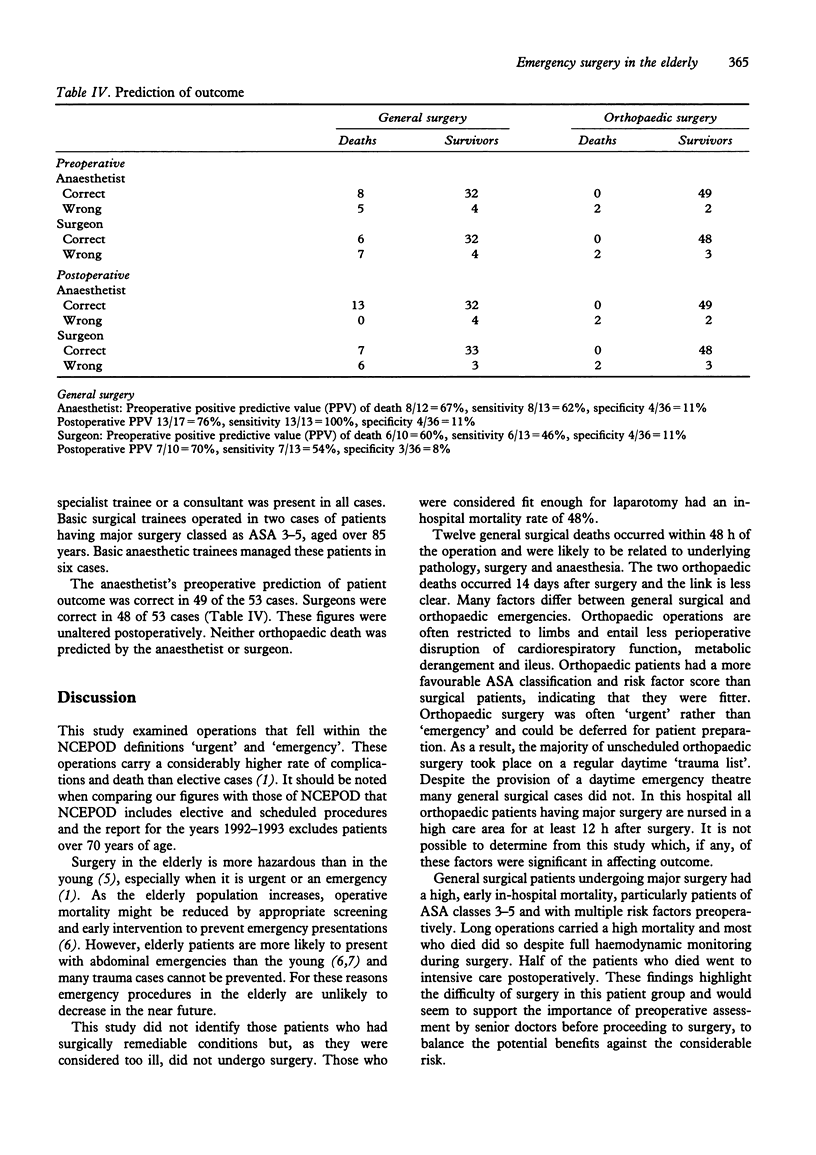
An audit was carried out of 102 patients aged over 75 years undergoing urgent or emergency surgery in a district general hospital. The risk of death in hospital after general surgery (13 deaths in 49 patients) was greater than after orthopaedic surgery (two deaths in 53 patients) (P < 0.05). In particular, laparotomy carried a high in-hospital mortality: 12 of 25 patients undergoing laparotomy died. Risk of death after general surgery increased with increasing preoperative ASA class, increasing medical risk factors and duration of operation. Orthopaedic cases were fitter than the general surgical cases as determined by ASA class and the number of medical risk factors. NCEPOD has recommended increased involvement of senior medical staff in operations, reduced night-time operating and avoidance of futile surgery. A high proportion of cases were operated on and anaesthetised by higher specialist trainees and consultants. Death rate was not affected by the seniority of doctors involved, nor by the time of day the operation took place. General surgical deaths were predictable postoperatively in most cases, but preoperative prediction of outcome was not specific enough to alter management.
Full text
PDF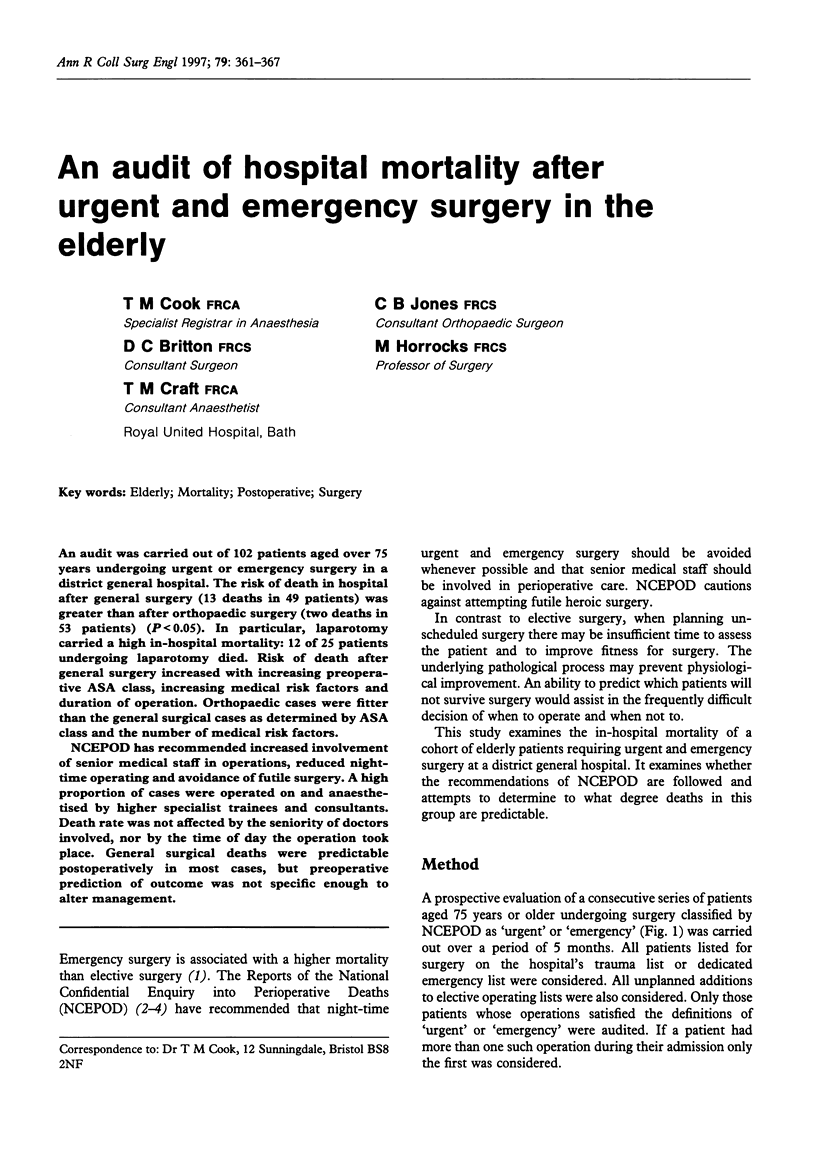
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Boyd O., Grounds R. M., Bennett E. D. A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk surgical patients. JAMA. 1993 Dec 8;270(22):2699–2707. [PubMed] [Google Scholar]
- Haynes S. R., Lawler P. G. An assessment of the consistency of ASA physical status classification allocation. Anaesthesia. 1995 Mar;50(3):195–199. doi: 10.1111/j.1365-2044.1995.tb04554.x. [DOI] [PubMed] [Google Scholar]
- Kennedy R. H., al-Mufti R. A., Brewster S. F., Sherry E. N., Magee T. R., Irvin T. T. The acute surgical admission: is mortality predictable in the elderly? Ann R Coll Surg Engl. 1994 Sep;76(5):342–345. [PMC free article] [PubMed] [Google Scholar]
- Lubin M. F. Is age a risk factor for surgery? Med Clin North Am. 1993 Mar;77(2):327–333. doi: 10.1016/s0025-7125(16)30254-1. [DOI] [PubMed] [Google Scholar]
- McIlroy B., Miller A., Copeland G. P., Kiff R. Audit of emergency preoperative resuscitation. Br J Surg. 1994 Feb;81(2):200–202. doi: 10.1002/bjs.1800810213. [DOI] [PubMed] [Google Scholar]
- Pedersen T., Eliasen K., Henriksen E. A prospective study of mortality associated with anaesthesia and surgery: risk indicators of mortality in hospital. Acta Anaesthesiol Scand. 1990 Apr;34(3):176–182. doi: 10.1111/j.1399-6576.1990.tb03066.x. [DOI] [PubMed] [Google Scholar]
- Seymour D. G., Pringle R. Surgical emergencies in the elderly: can they be prevented? Health Bull (Edinb) 1983 May;41(3):112–131. [PubMed] [Google Scholar]
- Waldron R. P., Donovan I. A., Drumm J., Mottram S. N., Tedman S. Emergency presentation and mortality from colorectal cancer in the elderly. Br J Surg. 1986 Mar;73(3):214–216. doi: 10.1002/bjs.1800730320. [DOI] [PubMed] [Google Scholar]