

Abstract
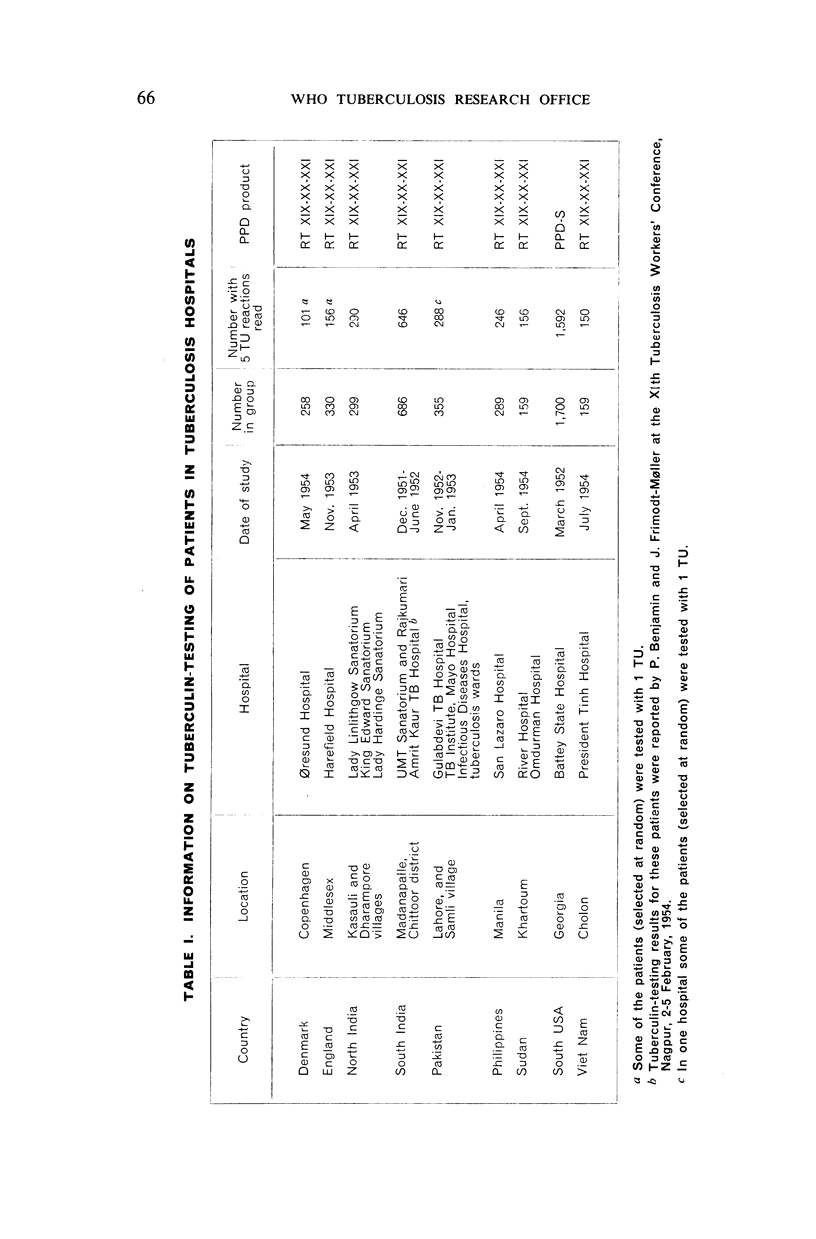
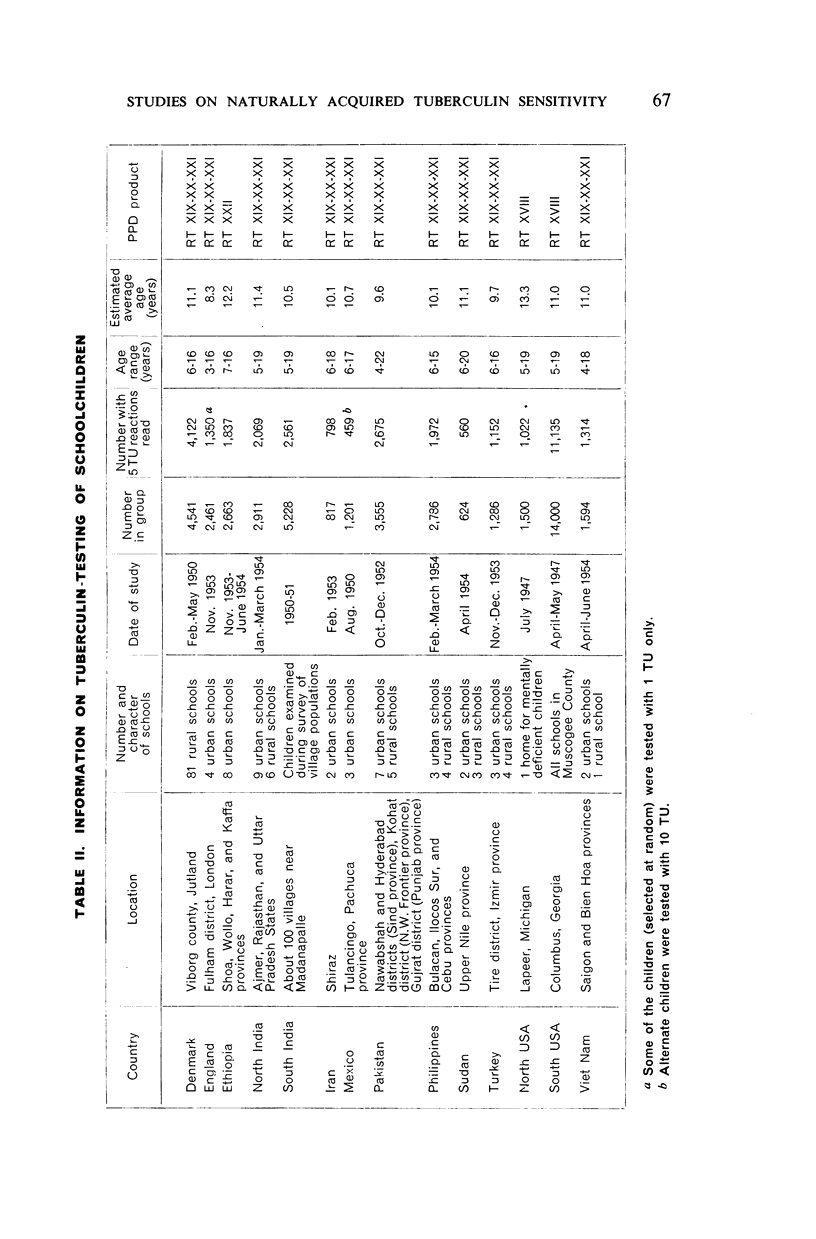
This paper presents the results of the tuberculin-testing of over 3,600 patients in tuberculosis hospitals and of nearly 34,000 schoolchildren in widely separated areas where arrangements could be made for specially trained personnel to work with uniform materials and techniques. Both patients and children were tested with an intradermal dose of 5 TU, and the children were retested with 100 TU if the reactions were less than 5 mm.
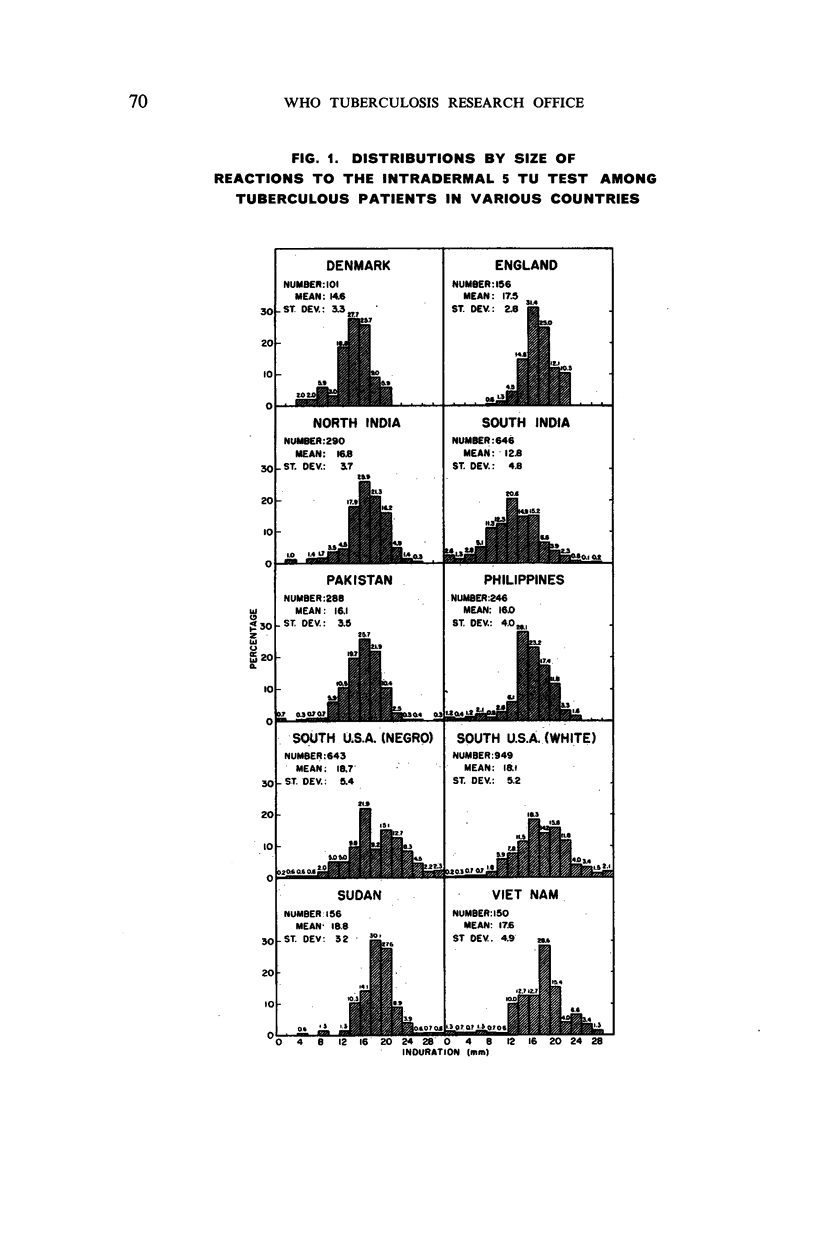
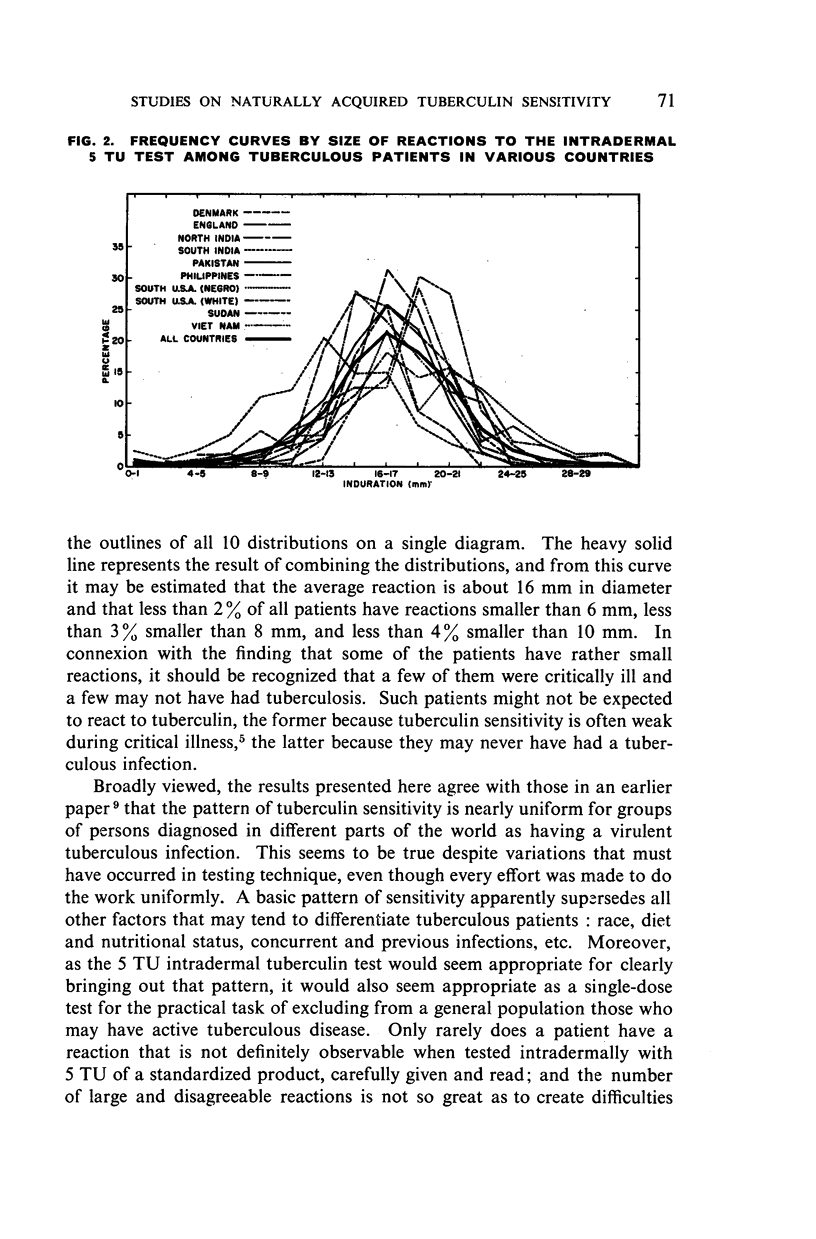
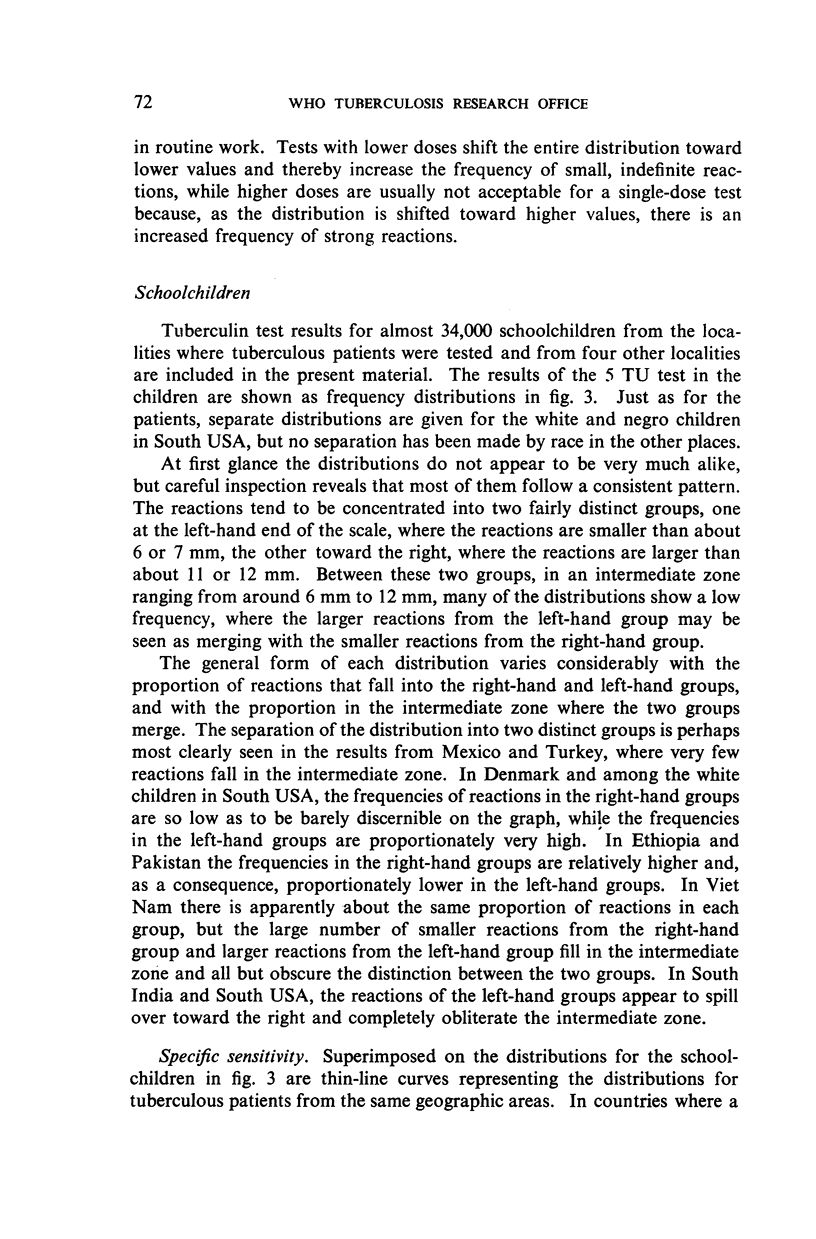
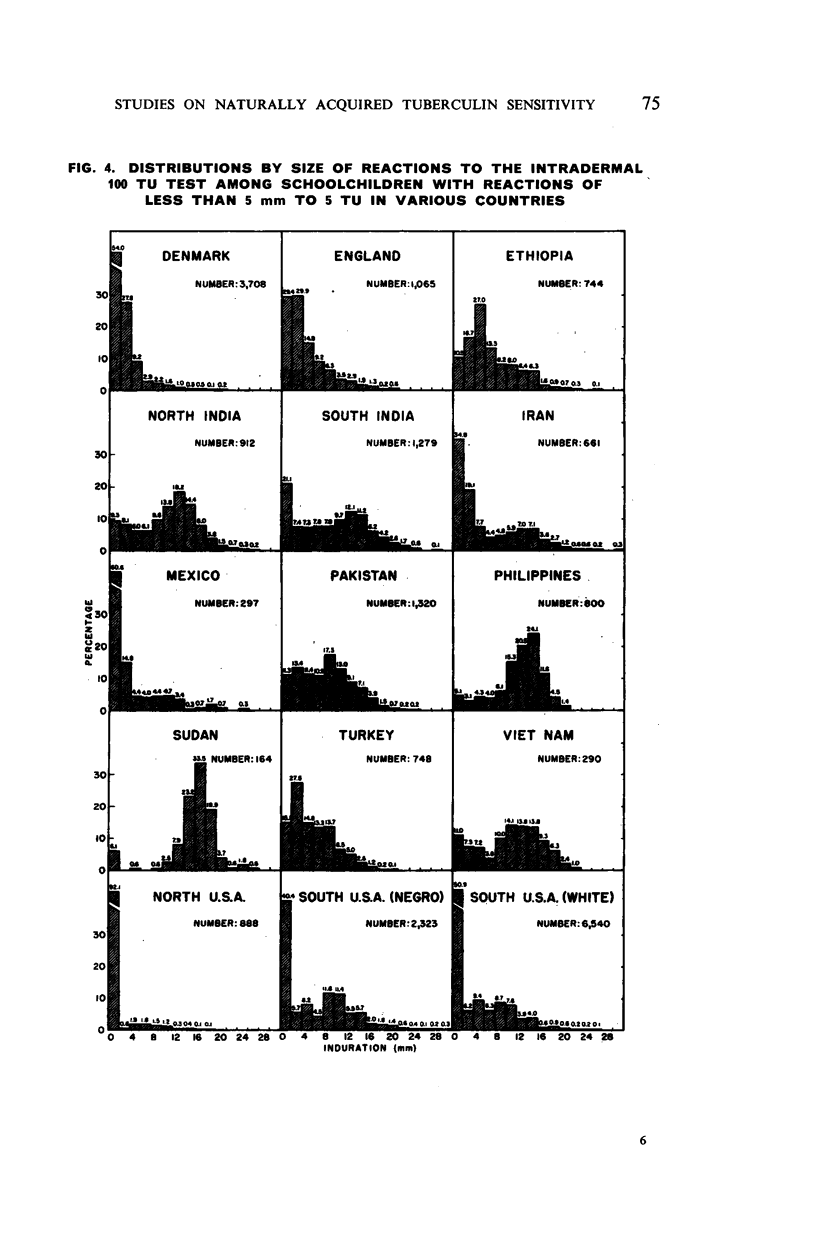
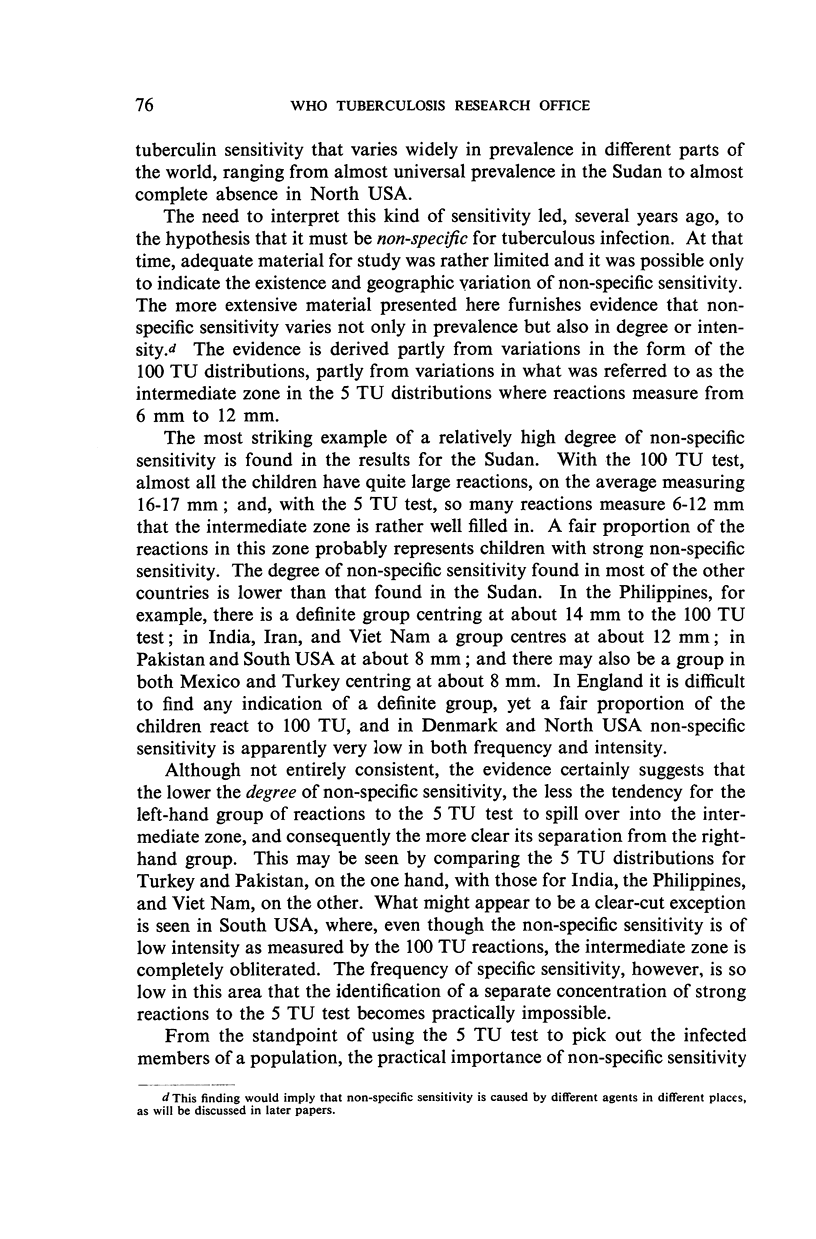
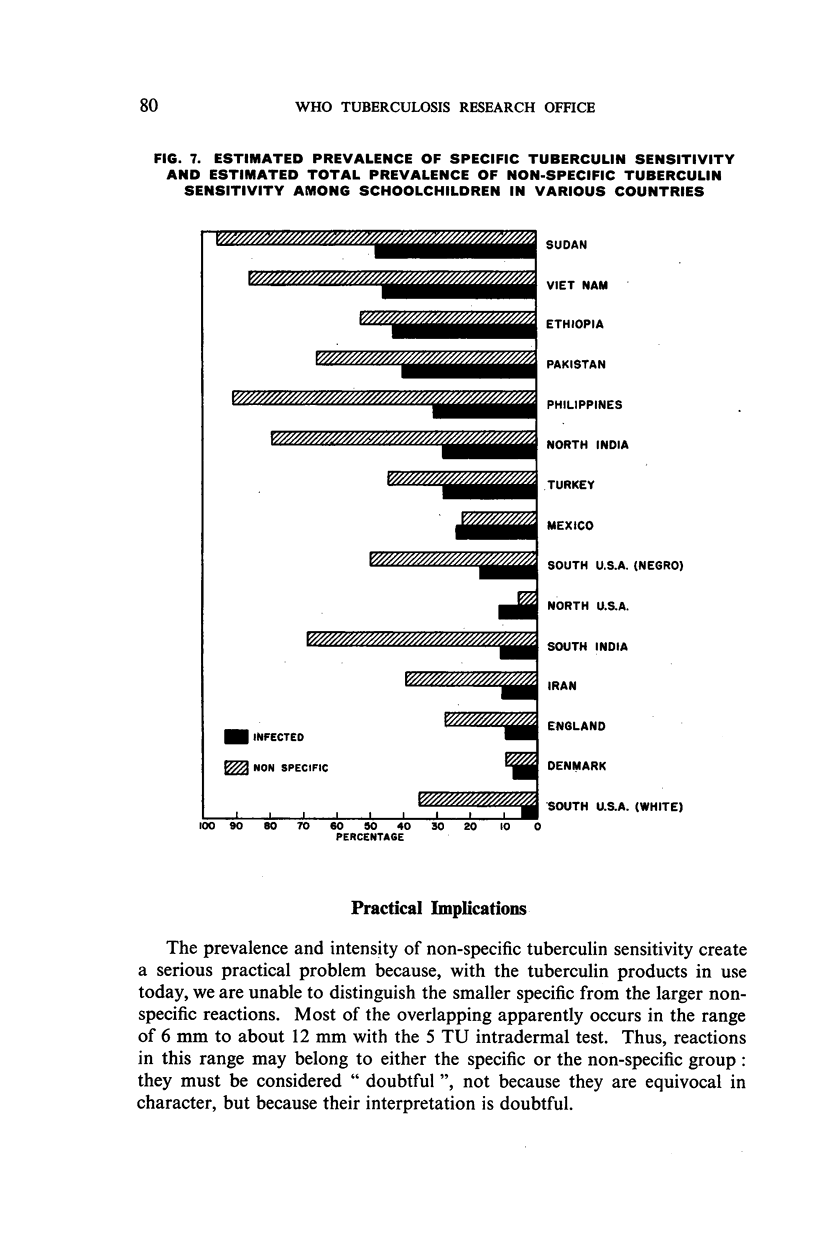
The results confirm those of earlier papers, that at least two different kinds of naturally acquired tuberculin sensitivity are found in many human populations: a high-grade sensitivity, designated as specific for virulent tuberculous infection, and a low-grade kind designated as non-specific, or not specific for tuberculous infection. Specific sensitivity is the kind found in tuberculous patients and in some schoolchildren everywhere. It follows a remarkably uniform pattern wherever it is found, apparently varying only in prevalence, not in degree, from place to place. In contrast, non-specific sensitivity varies both in prevalence and in degree. It ranges from nearly universal prevalence in some localities to almost complete absence in others, from a low degree to a relatively high degree approaching that of specific sensitivity. Non-specific sensitivity is not correlated with specific sensitivity and may have different causes in different places.
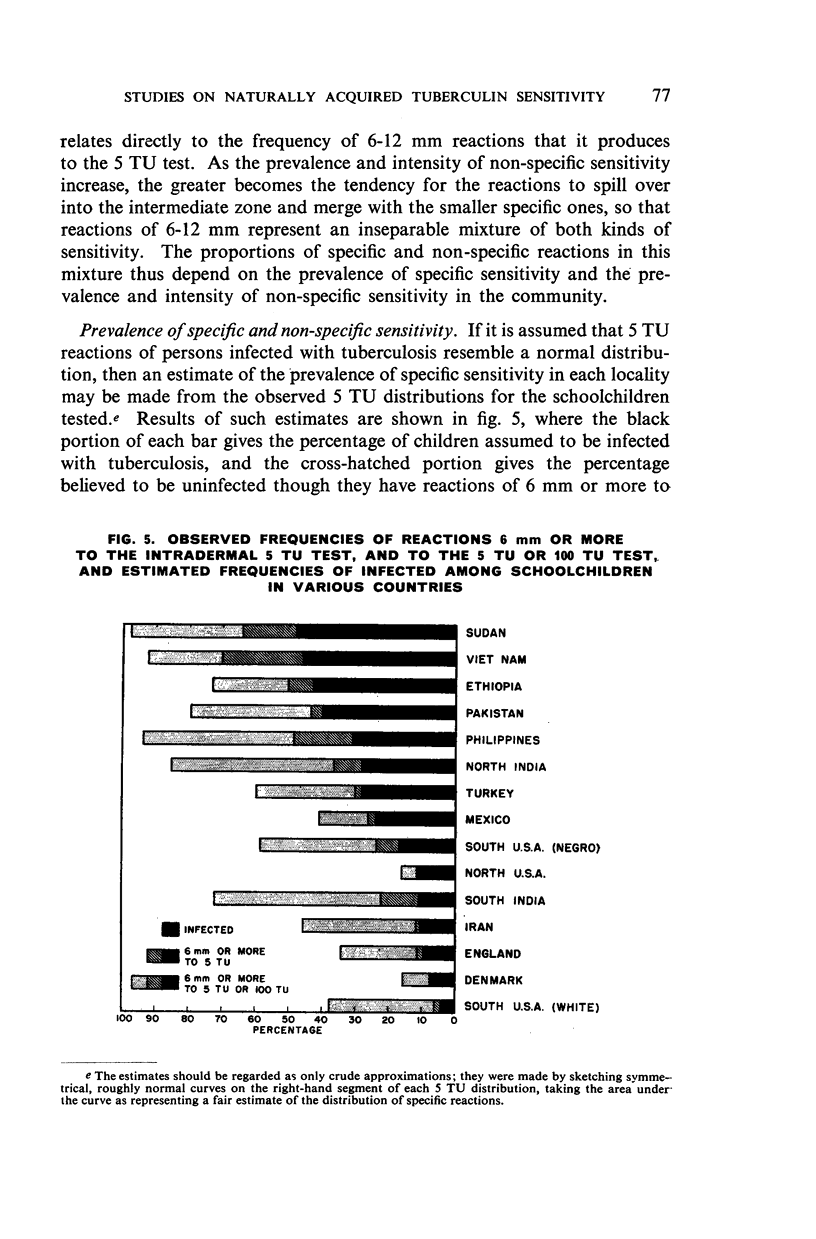
Serious practical problems are encountered as the prevalence and intensity of non-specific sensitivity increase, because the larger non-specific reactions cannot be distinguished from the smaller specific reactions with the tuberculin products in use today. A better, though not entirely satisfactory, separation of infected and uninfected persons might be obtained by using different criteria in different geographic areas for what is called a positive reaction to the 5 TU test. Changing the current criterion would probably provide a better estimate of the prevalence of infection in some communities: a lower proportion of the uninfected would be called positive at the expense of calling a few infected persons negative.
The analogous problem of separating specific from non-specific sensitivity in cattle has been provisionally solved by the veterinarians by comparative testing with tuberculins made from different types of mycobacteria. Similar methods are now being investigated for possible application to tuberculosis control work in human populations.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BATES L. E., BUSK T., PALMER C. E. Research contributions of BCG vaccination programs. II. Tuberculin sensitivity at different altitudes of residence. Public Health Rep. 1951 Nov 2;66(44):1427–1441. [PubMed] [Google Scholar]
- FENNER F. Studies on Mycobacterium ulcerans. II. Cross-reactivity in guineapigs sensitized with Mycobacterium ulcerans and other mycobacteria. Aust J Exp Biol Med Sci. 1952 Feb;30(1):11–20. [PubMed] [Google Scholar]
- PALMER C. E., BATES L. E. Tuberculin sensitivity of tuberculous patients. Bull World Health Organ. 1952;7(2):171–188. [PMC free article] [PubMed] [Google Scholar]
- PALMER C. E., MEYER S. N. Research contributions of BCG vaccination programs. I. Tuberculin allergy as a family trait. Public Health Rep. 1951 Mar 2;66(9):259–276. [PMC free article] [PubMed] [Google Scholar]
- PALMER C. E. Tuberculin sensitivity and contact with tuberculosis; further evidence of nonspecific sensitivity. Am Rev Tuberc. 1953 Nov;68(5):678–694. doi: 10.1164/art.1953.68.5.678. [DOI] [PubMed] [Google Scholar]