

Although scrotal inflation by saline infusion has been widely publicised on websites,1,2 this procedure has rarely been reported in the medical literature. We report an HIV positive man who presented with severe scrotal cellulitis following an infusion of saline into his scrotum. Clinicians should be aware of unusual causes of scrotal cellulitis and should warn patients about potential complications of this hazardous practice. To our knowledge, this has never previously been reported in an HIV positive patient.
Case report
A 52 year old homosexual white man, HIV positive since 1996, presented in April 2005 with a 2 day history of painful scrotal swelling. He had obtained information and a disposable scrotal infusion toolkit from a website3 and had infused 2½ litres of normal saline into his scrotum over 2 hours, 3 days previously. He had done this many times before without complications and the swelling had previously resolved over 2 days. On this occasion he sought medical advice because the pain and swelling had lasted for more than 3 days. He was on combination antiretroviral therapy with tenofovir, emtricitabine, and efavirenz. A recent HIV RNA level was undetectable and CD4 count was 443 cells ×106/l. Examination revealed a grossly swollen, erythematous, tender scrotum suggestive of severe cellulitis. Blood culture was not performed, as he was not systematically unwell and was afebrile. A Prince Albert ring and scars from previous infusions were also noted (fig 1). There was no inguinal lymphadenopathy or ulceration. The cellulitis resolved after a week's course of co‐amoxiclav 375 mg (amoxycillin 250 mg and clavulanic acid 125 mg) three times a day. Despite the severity of his illness, the patient declined to stop this practice and he was therefore advised on how to reduce the risk of complications. Advice included using alcohol swabs to clean the scrotum and to use Venflon (plastic needle in situ for infusion) rather than a metal needle that could damage surrounding soft tissue.

Figure 1 Shows previous infusion scars (arrow), Prince Albert ring, and marked cellulitis. (Reproduced with permission of patient.)
Discussion
Causes of painful scrotal swelling include torsion of the testis and its appendages, epididymitis, orchitis, incarcerated hernia, infarcted germ cell tumour, scrotal cellulites, and trauma. Our patient's swelling was self induced. Scrotal cellulitis as a complication of infusion of saline in a 37 year old man has previously been reported but his HIV status was not given.4 Gaseous inflation of the scrotum causing scrotal emphysema has also been recognised.5 A 51 year old white man developed mediastinal, retroperitoneal, and scrotal emphysema following scrotal inflation by his wife using a drinking straw.6 This can result in fatal air embolism. Fournier's gangrene (FG) can be a fatal complication of soft tissue injuries especially in HIV positive patients. In 1883, a French venereologist, Jean Alfred Fournier first reported synergistic necrotising faciitis leading to thrombosis of small subcutaneous vessels and resulting in gangrene of the penis and scrotum in young healthy males. He did not find the cause.7 The disease is not confined to young males, females can be affected too,8 and the source of the invasive infection can be localised to the colorectal or genitourinary tracts. FG has also been reported as a result of rectal and genitourinary trauma following instrumentation and surgical procedures. Superficial soft tissue injuries of the perineum account for the rest of the causes. In children, the causes of FG include trauma, insect bites, burns, perirectal infections, and systemic infections.9
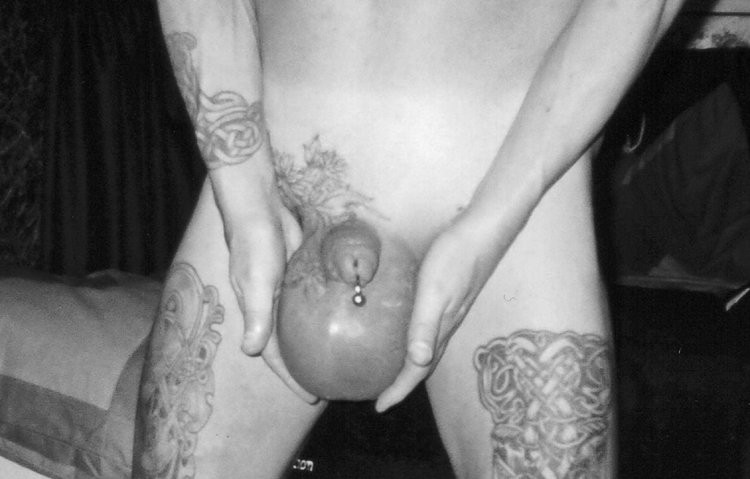
Figure 2 Showing diffuse symmetrical tense scrotal swelling. Photograph taken by the patient's friend on a previous occasion. (Reproduced with permission of patient.)
Most patients who develop FG usually have predisposing factors such as diabetes mellitus, alcoholism, advanced age, malnutrition, and HIV infection.10 The first case of FG in an HIV positive male as a result of injecting intravenous drugs into his femoral veins was reported in 1991.11
Patients should be educated about the dangers of inflation procedures of scrotum and strongly discouraged from doing it. β Haemolytic streptococci cause the majority of scrotal cellulitis cases.12 Other bacterial causes of cellulitis include staphylococci, coliforms, clostridium, and anaerobes including Bacteroides fragilis and Prevotella, Porphyromonas, and Actinomyces sp.13 Emphysematous genital infection caused by Candida albicans has also been reported.14 Low virulence organisms such as Lactobacillus gasseri causing FG have also been described.15 Congenital penoscrotal lymphoedema complicated by cellulitis, lymphangitis, and severe sepsis caused by a streptococcal infection has been reported.16 Rare causes of scrotal swelling due to cutaneous Crohn's disease presenting with erythematous non‐tender swelling of the scrotum have been reported in young males.17 This shows the importance of obtaining a detailed clinical history and careful attention to physical signs. Likewise, clinicians should be aware of unusual sex practices18 and associated possible rare causes of scrotal cellulitis. Careful examination, including looking for any needlestick marks, is essential in patients with marked scrotal swelling since some may not admit to this procedure.
References
- 1. www.eBay
- 2. www.bmezine.com
- 3. www.chaseunion.com
- 4.Summers A J. A complication of an unusual sexual practice. South Med J 200396716–717. [DOI] [PubMed] [Google Scholar]
- 5.Sharma T C, Kagan H N. Scrotal emphysema. Am Surg 198046652–653. [PubMed] [Google Scholar]
- 6.Bush G, Nixon R K. Scrotal inflation. A new cause for subcutaneous, mediastinal and retroperitoneal emphysema. Henry Ford Hosp Med J 196917225–226. [PubMed] [Google Scholar]
- 7.Laucks S S. Fournier's gangrene. Surg Clin N Am 1994741339–1352. [DOI] [PubMed] [Google Scholar]
- 8.Stephens B J, Lathrop J C, Rice W T.et al Fournier's gangrene: historic (1764–1978) verses contemporary (1979–1988) differences in etiology and clinical importance. Am Surgeon 199359149–154. [PubMed] [Google Scholar]
- 9.Patankar S P, Lalwani S K. Fournier's gangrene. Indian Paediatrics 200441511. [PubMed] [Google Scholar]
- 10.Paty R, Smith A D. Gangrene and Fournier's gangrene. Urol Clin N Am 199219149–162. [PubMed] [Google Scholar]
- 11.Murphy M, Buckley M, Corr J.et al Fournier's gangrene of scrotum in a patient with AIDS. Genitourin Med 199167339–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Haury B, Rodeheaver G, Stevenson T.et al Streptococcal cellulitis of the scrotum and penis with secondary skin gangrene. Surg Gynecol Obstet 197514135–39. [PubMed] [Google Scholar]
- 13.Brook I. Urinary tract and genito‐urinary suppurative infections due to anaerobic bacteria. Int J Urol 200411133–141. [DOI] [PubMed] [Google Scholar]
- 14.Humayun H, Maliwan N. Emphysematous genital infection caused by Candida albicans. J Urol 19821281049–1050. [DOI] [PubMed] [Google Scholar]
- 15.Tleyjeh I M, Routh J, Qutub M O.et al Lactobacillus gasseri causing Fournier's gangrene. Scan J Infect Dis 200436501–503. [DOI] [PubMed] [Google Scholar]
- 16.Watanabe, Toru Congenital penoscrotal lymphedema complicated by sepsis associated with a streptoccal infection. Pediatric Emergency Care 200016423–425. [DOI] [PubMed] [Google Scholar]
- 17.Acker S M, Sahn E E, Rogers H C.et al Genital cutaneous Crohn disease: two cases with unusual clinical and histopathologic features in young men. Am J Dermatopathol 200022443–446. [DOI] [PubMed] [Google Scholar]
- 18.Love B.The encyclopaedia of unusual sex practices. Fort Lee, NJ: Barricade Books, 1995