
FIG. 2.
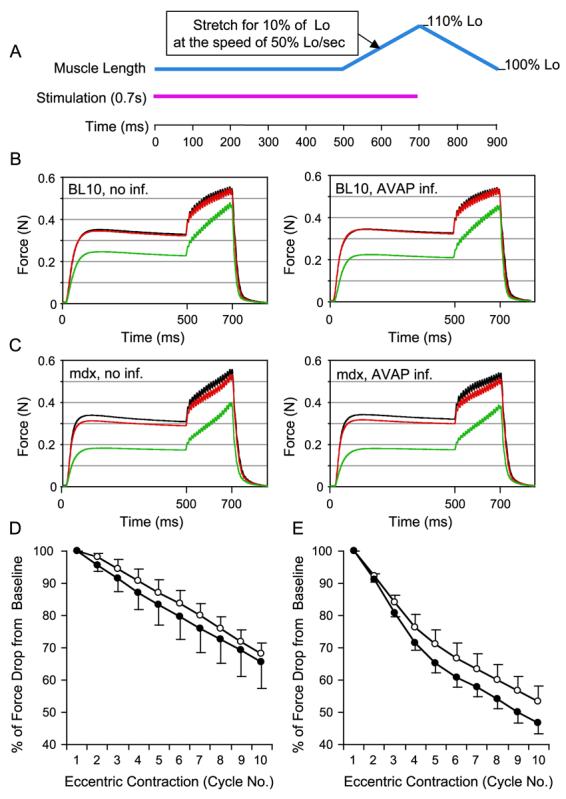
AV.RSV.AP infection did not aggravate eccentric contraction-induced injury in the EDL muscle. (A) Schematic outline of the eccentric contraction protocol used in this study. Muscle was stimulated at 150 Hz for 700 ms (pink line). At the beginning of the stimulation, muscle length (blue line) was adjusted to the optimal length (Lo). At the end of 500 ms stimulation, muscle length was stretched to 110% of Lo at the speed of 50% Lo/s. At the end of stimulation, muscle length was returned to Lo at the same speed. A total of 10 stretch (eccentric contraction) cycles were performed in each muscle. An isometric tetanic force was developed during the first 500 ms stimulation. The change of this tetanic force between each eccentric contraction cycle reflected the degree of muscle injury. (B) Representative force tracing in BL10 EDL muscles. Left, without AAV infection; right, infected with AV.RSV.AP. Black line, force tracing from the first cycle. Red line, force tracing from the second cycle. Green line, force tracing from the 10th cycle. (C) Representative force tracing in mdx EDL muscles. Left, without AAV infection; right, infected with AV.RSV.AP. Black line, force tracing from the first cycle. Red line, force tracing from the second cycle. Green line, force tracing from the 10th cycle. The isometric tetanic force drop was more significant in mdx muscles. However, there was no significant difference between the AV.RSV.AP-infected muscle and the saline-injected control. (D) Relative change in tetanic force during 10 cycles of eccentric contraction in BL10 EDL muscles (N = 4 pairs). The tetanic tension developed during the first cycle was designated as 100%. Open circle, without AAV infection (mean + SEM). Closed circle, infected with AV.RSV.AP (mean − SEM). (E) Relative change of tetanic force during 10 cycles of eccentric contraction in mdx EDL muscles (N = 5 pairs). The isometric tetanic tension developed during the first cycle was designated as 100%. Open circle, without AAV infection (mean + SEM). Closed circle, infected with AV.RSV.AP (mean − SEM). AV.RSV.AP infection resulted in a slightly bigger, but not statistically significant, force deficit in the last few cycles. (For interpretation of the references to color in this figure legend, the reader is referred to the web version of this article.)