

Abstract
A 31-year-old male was presented with a very rare case of ipsilateral palsies of the nerves IX through XII (Collet-Sicard syndrome) after a closed head injury. An occipital condyle fracture that was associated with epidural hematoma was diagnosed by computed tomography. The patient was conservatively managed, and following the treatment, partial neurological recovery ensued. The phenomenon of occipital condyle fracture involving the last four cranial nerve palsies is relatively rare. Although 3 cases of Collet-Sicard syndrome that were caused by an occipital condyle fracture has been reported, the association between condyle fracture and epidural hematoma has never been described before.
Keywords: Collet-Sicard syndrome, cranial nerve palsy, epidural hematoma, occipital condyl fracture
INTRODUCTION
Unilateral paralysis of the last four cranial nerves (IX-XII) is referred to as the "Collet-Sicard syndrome".1,2 This syndrome can be caused in many different ways. Malignant lesions of the skull base and nasopharynx are more frequent causes.3,4 Occipital condyle fracture (OCF) is a very rare traumatic lesion of the skull base, that causes lower cranial nerve damage.5-8 Most craniocervical junction injuries, including OCF, are sustained in high-speed motor vehicle accidents or in a fall from a great height, and; they usually result in instantaneous death. In the available literature only 3 cases of Collet-Sicard syndrome had been reported that has been caused by an occipital condyle fracture after a closed head injury.9-11 We describe a case of Collet-Sicard syndrome, which developed after and is associated with the closed head injury that includes the occipital condyle fracture and epidural hematoma, and discuss the mechanisms, diagnosis, and treatment of this rare lesion are also discussed.
CASE REPORT
A 31-year-old man suffered from a closed head trauma in a motor vehicle accident. The cervical collar was applied in the ambulance during his transport to the hospital. At the time of admission, he was drowsy with a Glasgow Coma Score of 14. On examination, tenderness on the occipitocervical region, and swallowing difficulty and weakness on right shoulder elevation were apparent. A right vocal cord paralysis was noted during indirect laryngoscopy. His right gag reflex was absent, and his voice was hoarse with a nasal twang. The right trapezius and sternocleidomastoid muscles were apparently weak, otherwise the patient was neurologically intact. A right lung pneumothorax was identified by both a standard graphies and a physical examination. Standard x-ray films of the cranial and cervical regions were normal. An axial computed tomography (CT) scan of the skull base showed minimal brain edema and an avulsion fracture of the right occipital condyle that was associated with an epidural hematoma between the bone fragment and the dens of the atlas (Fig. 1). A coronal CT scan with the bone window illustrated a medial and cranial displacement of the bone fragment (Fig. 2). The patient was conservatively treated and was placed in a halo brace. A chest tube was placed in the pneumothorax, and the nasogastric tube was inserted for feeding. The patient was discharged home on day 50 and did not have any swallowing difficulty, but the dysphonia has persisted. Sixteen months after the injury, the vocal cord paralysis and the slight tongue deviation to the left was still present. The patient was able to swallow, and there was a marked awkward of his right trapezius.
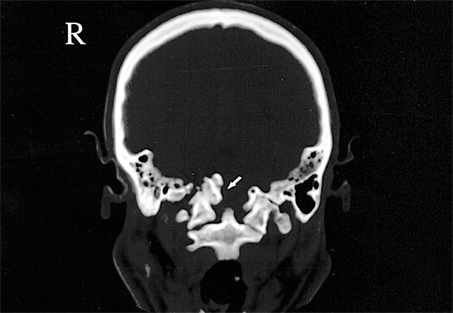
Fig. 1.

An axial computed tomography scan showed an avulsion fracture of the right occipital condyle (short arrow) associated with epidural hematoma (long arrow) between the bone fragment and dens of atlas.
Fig. 2.
A coronal computed tomography scan with the bone window showed medial and cranial displacement of the bone fragment (arrow).
DISCUSSION
A syndrome consisting of unilateral lesions of the last four cranial nerves was first described by Collet1 and Sicard2 and is now called the Collet Sicard syndrome. This syndrome has been described in association with the Jefferson fracture,12 idiopathic cranial polyneuropathy,13 multiple myeloma,14 internal carotid artery dissection,15 and coiling,16 Lyme disease,17 and also in association with skull base tumors of primary and metastatic (prostate, lung, breast, and renal tumors) origin.3-6 One of the rare causes of the Collet-Sicard syndrome is the occipital condyle fractures.9-11 Although they are among the more rare traumatic lesions of the skull base and have received little attention, occipital condyle fractures constitute an anatomoclinical entity because of their special features. Occipital condyles are in close relationship with the hypoglossal canal and the jugular foramen, which includes the cranial nerves IX, X, and XI. Occipital condyles also have a vital anatomical relationship to the brain stem and vascular structures.
Type I injury occurs secondary to an axial load injury of the occipital condyle, resulting in comminution and impaction. Most importantly, the tectorial membrane and alar ligaments are weakened, but not ruptured, and the overall anatomic stability is preserved. Type II injuries occur after a blunt trauma to the occiput with a fracture of the occipital condyle propagating into the foramen magnum. Such a basilar skull fracture may involve one or both occipital condyles, and the skull is typically stable due to an intact tectorial membrane and/or an atlantal ligament. Type III essentially describes an avulsion fracture of the inferomedial portion of the condyle, which is most probably the result of the inertia of the head caused by craniocervical hyperextension or hyperflexion. Stability of the occipito-cervical region is maintained by the cruciate ligament, the apical dental ligament, the paired alar ligaments, and the tectorial membrane.5,18 An injury of the alar ligaments and the tectorial membrane usually result in an avulsion fracture of the occipital condyle, also commonly involving the anterior margin of the foramen magnum. Because sheer or rotational forces are usually responsible for these injuries, a ligamentous injury is more likely to result, and this can,in turn, cause atlantooccipital dislocation, subluxation, or the potential for severe instability. Tuli et al.19 later modified this classification. Considering the relationship of the occipital condyle to the jugular foramen in terms of the cranial nerves IX, X, and XI and to the hypoglossal canal with nerve XII, it is not difficult to imagine how an OCF can produce lower cranial nerve damage. Cranial nerve palsies may result from nerve compression, nerve stretching, or nerve rootlet avulsion.
The clinical presentation of the Collet Sicard syndrome is highly variable. OCF can cause nerve palsies,7 most of which are of late onset, probably due to fragment migration and callus formation. Immediate onset of cranial nerve palsies after injury, as in our case, is rare. Clinically, this syndrome is characterized by hoarseness of the voice, and difficulty in swallowing, and unclear speech. Early detection of this syndrome may be difficult in patients with head injuries because of their altered state of consciousness. Demonstration of skull base fractures or fractures involving the exit foramina may be very difficult with conventional radiographic techniques alone.2,20 Plain radiographs of the cervical spine showed no traumatic lesions in our patient. CT, with the window level set for bone visualization, are the most useful methods for demonstrating these fractures as in our case.20 With conventional radiography, a soft-tissue shadow seen in the nasopharynx may be indirect evidence of these skull base fractures.
Although OCFs were initially reported in a patient who sustained severe head trauma and had severe neurologic deficits,8 many cases of patients with a normal level of consciousness have also been reported.21 This stresses the fact that OCF must be considered even if the consciousness of the patient is normal.
Fuentes et al.22 reported a case of a bilateral occipital condyle fracture with clival epidural hematoma. In a similar article, Miyazaki et al.23 reported a case of an occipital condyle fracture with multiple nerve palsies and a thick hematoma in the prepontine cistern. In our case, an epidural hematoma was seated very close to the bone fragment.
Occipital condylar fractures usually heal quite well with conservative therapy, e.g., nasogastric tube feeding, prophylactic antibiotics, and physiotherapy. Patients with respiratory distresses may need tracheostomy.11,24 Recovery is slow, and residual neurologic deficits may persist for a long time. Only rarely is surgical fusion required. The treatment of occipital condyle fractures depends on a variety of factors, which include the occurrence of other injuries, the patient's neurological condition, and the type of occipital fracture present. Type II fractures are relatively stable, and patients with these lesions may be treated with immobilization in a hard collar for 2 to 3 months. Type I and III occipital fractures can be unstable, and although such injuries have been treated with a hard collar in the past, immobilizing the patient with a halo vest appears to be more appropriate.19
We believe fractures of the occipital condyle are more common than is reported. With patients, who have, sustained a severe head injury with evidence of lower cranial nerve palsy and with patients with continued neck pain but have no abnormalities shown in their radiographs, the possibility of OCF should be investigated. Axial and coronal CT scanning with bone windows are extremely useful methods for demonstrating these fractures.
References
- 1.Collet FJ. Sur un nouveau syndrome paralytique pharyngolarynge par blessure de guerre (Hemiplegie glosso-laryngo-scapulopharyngee) Lyon Med. 1915;124:121–129. [Google Scholar]
- 2.Sicard JA. Syndrome du carrefour condylo-dechire posterieur (type pur de paralysie laryngee associee) Marseille Med. 1917;53:383. [Google Scholar]
- 3.Comacchio F, D'Eredita R, Poletto E, Poletti A, Marchiori C. Hemangiopericytoma of the skull base and Collet-Sicard syndrome: a case report. Ear Nose Throat J. 1995;74:845–847. [PubMed] [Google Scholar]
- 4.Mohanty SK, Barrios M, Fishbone H, Khatib R. Irreversible injury of cranial nerves 9 trough 12 (Collet-Sicard syndrome). Case report. J Neurosurg. 1973;38:86–88. doi: 10.3171/jns.1973.38.1.0086. [DOI] [PubMed] [Google Scholar]
- 5.Anderson PA, Montesano PX. Morphology and treatment of occipital condyle fractures. Spine. 1988;13:731–736. doi: 10.1097/00007632-198807000-00004. [DOI] [PubMed] [Google Scholar]
- 6.Bolender N, Cromwell LD, Wendling L. Fracture of the occipital condyle. AJR Am J Roentgenol. 1978;131:729–731. doi: 10.2214/ajr.131.4.729. [DOI] [PubMed] [Google Scholar]
- 7.Ide C, Nisolle JF, Misson N, Trigaux JP, Gustin T, De Coene B, et al. Unusual occipitoatlantal fracture dissociation with no neurological impairment. Case report. J Neurosurg. 1998;88:773–776. doi: 10.3171/jns.1998.88.4.0773. [DOI] [PubMed] [Google Scholar]
- 8.Orbay T, Aykol S, Seckin Z, Ergun R. Late hypoglossal nerve palsy following fracture of the occipital condyle. Surg Neurol. 1989;31:402–404. doi: 10.1016/0090-3019(89)90076-1. [DOI] [PubMed] [Google Scholar]
- 9.Hashimoto T, Watanabe O, Takase M, Koniyama J, Kobota M. Collet-Sicard syndrome after minor head trauma. Neurosurgery. 1988;23:367–370. doi: 10.1227/00006123-198809000-00015. [DOI] [PubMed] [Google Scholar]
- 10.Sharma BS, Mahajan RK, Bhatia S, Khosla VK. Collet-Sicard syndrome after closed head injury. Clin Neurol Neurosurg. 1994;96:197–198. doi: 10.1016/0303-8467(94)90063-9. [DOI] [PubMed] [Google Scholar]
- 11.Wani MA, Tandon PN, Banerji AK, Bhatia R. Collet-Sicard syndrome resulting from closed head injury: case report. J Trauma. 1991;31:1437–1439. doi: 10.1097/00005373-199110000-00025. [DOI] [PubMed] [Google Scholar]
- 12.Connolly B, Turner C, DeVine J, Gerlinger T. Jefferson fracture resulting in Collet-Sicard syndrome. Spine. 2000;25:395–398. doi: 10.1097/00007632-200002010-00023. [DOI] [PubMed] [Google Scholar]
- 13.Juncos JL, Beal MF. Idiopathic cranial polyneuropathy. A fifteen-year experience. Brain. 1987;110:197–211. doi: 10.1093/brain/110.1.197. [DOI] [PubMed] [Google Scholar]
- 14.Tappin JA, Satchi G, Corless JA, Ashworth F. Multiple myeloma presenting as the Collet-Sicard syndrome. J Neurol Neurosurg Psychiatry. 1996;60:14. doi: 10.1136/jnnp.60.1.14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rees JH, Valentine AR, Llewelyn JG. Spontaneous bilateral carotid and vertebral artery dissection presenting as a Collet-Sicard syndrome. Br J Radiol. 1997;70:856–858. doi: 10.1259/bjr.70.836.9486056. [DOI] [PubMed] [Google Scholar]
- 16.Silvestrini M, Floris R, Tagliati M, Stanzione P, Simonetti G. Collet-Sicard syndrome caused by a coiling of the internal carotid artery. Riv Neurol. 1991;61:135–136. [PubMed] [Google Scholar]
- 17.Pachner AR, Steere AC. The triad of neurologic manifestations of Lyme disease: meningitis, cranial neuritis, and radiculoneuritis. Neurology. 1985;35:47–53. doi: 10.1212/wnl.35.1.47. [DOI] [PubMed] [Google Scholar]
- 18.Bridgman S, McNab W. Traumatic occipital condyle fracture, multiple cranial nerve palsies, and torticollis: a case report and review of the literature. Surg Neurol. 1992;38:152–156. doi: 10.1016/0090-3019(92)90094-4. [DOI] [PubMed] [Google Scholar]
- 19.Tuli S, Tator CH, Fehlings MG, Mackay M. Occipital condyle fractures. Neurosurgery. 1997;41:368–377. doi: 10.1097/00006123-199708000-00006. [DOI] [PubMed] [Google Scholar]
- 20.DiChiro G, Fisher RL, Nelson KB. The jugular foramen. J Neurosurg. 1964;21:447–460. doi: 10.3171/jns.1964.21.6.0447. [DOI] [PubMed] [Google Scholar]
- 21.Bucholz RW, Burkhead WZ, Graham W, Petty C. Occult cervical spine injuries in fatal traffic accidents. J Trauma. 1979;19:768–771. doi: 10.1097/00005373-197910000-00009. [DOI] [PubMed] [Google Scholar]
- 22.Fuentes S, Bouillot P, Dufour H, Grisoli F. Occipital condyle fractures and clivus epidural hematoma. Case report. Neurochirurgie. 2000;46:563–567. [PubMed] [Google Scholar]
- 23.Miyazaki C, Katsume M, Yamazaki T, Aoki K, Kuroki T, Takasu N. Unusual occipital condyle fracture with multiple nerve palsies and Wallenberg syndrome. Clin Neurol Neurosurg. 2000;102:255–258. doi: 10.1016/s0303-8467(00)00109-8. [DOI] [PubMed] [Google Scholar]
- 24.Grundy DJ, McSweeney T, Jones HW. Cranial nerve palsies in cervical injuries. Spine. 1984;9:339–343. doi: 10.1097/00007632-198405000-00002. [DOI] [PubMed] [Google Scholar]