
Fig. 2.
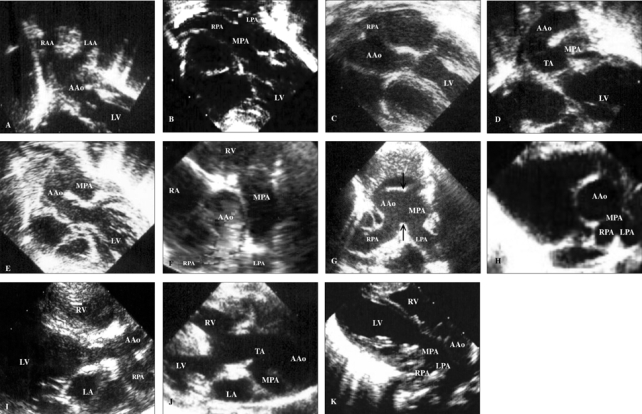
Subcostal view of the left ventricular outflow tract of echocardiography showed a characteristic morphology of the aortic bifurcations in cases with DAA (A), which has a longer bifurcation distance (from the semilunar valve to the site of bifurcation) than the bifurcation distance measured in cases with d-TGA (B), HTA (C), type I TA (D), and APW (E). Parasternal short-axis view showed an anomalous origin of the right pulmonary artery from the ascending aorta in a case of isolated HTA (F), and when complexed with APW (arrows) in the Berry syndrome (G), as well as an abnormal take-off of the main pulmonary artery from the left-posterior aspect of the aorta in cases with type I TA (H). Over the parasternal long-axis views, we may visualize bifurcation either from the ascending aorta, as in the case of HTA (I), or from the truncus in TA cases (J), which can be similar to d-TGA cases (K). AAo, ascending aorta; APW, aortopulmonary window; DAA, double aortic arch; d-TGA, dextro-transposition of the great arteries; HTA: hemitruncus arteriosus; LA, left atrium; LAA, left aortic arch; LPA, left pulmonary artery; LV, left ventricle; MPA, main pulmonary artery; RA, right atrium; RAA, right aortic arch; RPA, right pulmonary artery; TA, truncus arteriosus.