
Fig 2.
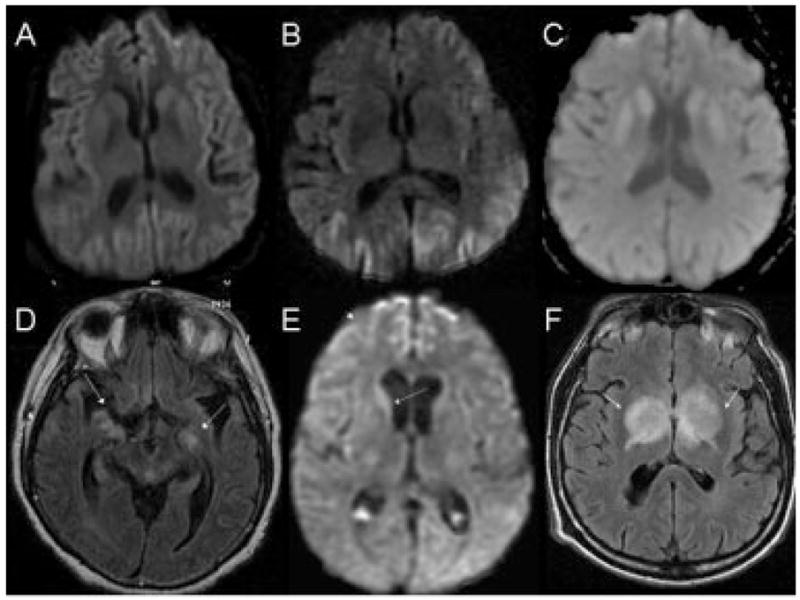
Brain magnetic resonance images (MRIs) in sporadic Creutzfeldt–Jakob disease (CJD) (A–C) and nonprion rapidly progressive dementias (RPDs) (D–F). Sporadic CJD axial diffusion-weighted imaging (DWI) with both cortical and striatal hyperintensity (A), only cortical (cortical ribboning) hyperintensity (B), and only striatal hyperintensity (C). Fluid-attenuated inversion recovery (FLAIR) MRIs (not shown) showed less hyperintensity than DWI sporadic CJD. Axial FLAIR MRI of patient with pathology-proved meningoencephalitis (D) showing extensive, patchy, T2-weighted white matter hyperintensity (arrows) that was variably contrast enhancing (not shown). Enterovirus was identified through the California Encephalitis Project by reverse transcription-polymerase chain reaction of brain biopsy tissue. DWI axial MRI of a patient with systemic sarcoid (E). Initial diagnosis suggested CJD because of caudate hyperintensity (arrow) and right frontal cortical ribboning (arrowhead). The apparent diffusion coefficient map (not shown), however, did not suggest restricted diffusion, and a lung node biopsy showed sarcoid. Axial FLAIR MRI of an RPD patient with parkinsonism (F). Arrows point to the masses in the bilateral deep nuclei. Note the mass effect with edema (arrows). The lesions were hypodense on T1 and showed some gadolinium enhancement (not shown). Brain biopsy showed a B-cell primary central nervous system lymphoma.