

Abstract
Purpose
Various pin configurations are possible to stabilize a supracondylar fracture. While cross pinning gives the best stabilty the disadvantage is the risk of iatrogenic ulnar nerve injury. We combine a cross pin fixation with a lateral approach. The aim of the study was to prove our method retrospectively to show the advantage of lateral cross-pinning achieving stabilty and avoiding ulnar nerve injury.
Method
Between 1 January 2001 and 31 December 2002, 84 supracondylar fractures were treated with invasive surgical procedure. The intention was a primary closed reduction. Following closed reduction under general anaesthesia, two K-wires were introduced from the lateral side, one ascending and the other descending. If it was not possible to perform a closed reduction, an open reduction was performed by medial–lateral crossed K-wire fixation. After either an open or closed reduction, the pins were buried under the skin. The results were evaluated using Flynn’s score. The mean time of follow-up was 18.9 months.
Results
Seventy-seven percent of the patients were treated with a closed reduction, while 23% needed an open reduction. A clinical follow-up examination was done at an average of 18.9 months following the trauma. Of those treated with a closed reduction alone, 93% had an excellent or good functional result. Of those requiring an open reduction, 88% had excellent or good result. None of our patients exhibited secondary dislocation or iatrogenic ulnar palsies.
Conclusion
Closed reduction and lateral crossed pin fixation with ascending and descending K-wires buried under the skin is an effective method to treat type II and III supracondylar fractures in children. The method gives stability and avoids iatrogenic ulnar nerve injuries.
Keywords: Supracondylar fractures, Closed reduction, Crossed-pin fixation
Introduction
Anywhere from 4 to 6.5% of all pediatric fractures are supracondylar fractures [1]. Closed reduction and percutaneous pinning are now widely accepted throughout the English- and French-speaking literature [2, 3, 4, 5, 6], while open reduction and pinning is still more commonly practiced in Germany [7]. There are various options for the pattern of K-wire fixation of displaced supracondylar fractures. Zionts et al. [8] measured the biomechanical stability of different fixations of adult human cadaver models. They found the greatest resistance to rotation occurred with medial–lateral cross pinning. The second most stable pattern was fixation utilizing three lateral diverging pins. The least stable was fixation with two lateral pins, which crossed at the fracture site. While medial–lateral cross pinning has the greatest resistance; the disadvantage is the risk of ulnar nerve injury [9, 10, 11, 12]. To achieve stability and avoid ulnar nerve injury we combine cross pinning and lateral pinning. The present study shows results of closed reduction and percutaneous pinning using a lateral cross-pinning technique.
Materials and methods
In a retrospective study patients with operatively treated supracondylar fractures were evaluated. Gartland’s classification was utilized [13]. Between January 2001 and 31 December 2002, 84 type III and II fractures were treated with invasive surgical procedures. Our standard treatment was to perform a closed reduction followed by lateral cross pin fixation. Treatment was performed as soon as possible after the initial trauma. The attending surgeon’s initial intention was to perform a closed reduction. Open reduction was performed when the fracture could not be satisfactorily reduced closed. In cases of pulselessness we first preformed a close reduction. In cases of negative Doppler ultrasound after closed reduction, the closed reduction followed an open procedure. In five cases the attending surgeons opted for a primary open reduction because of swelling and soft-tissue problems. The operations were done by four attending surgeons. Patients are excluded in cases of open fracture, fracture older than three days and when the patients had first treatment in another hospital. Patients younger than 15 years old were included.
The mean age was 6.5 years (range 2–13 years 8 months). Forty-nine patients were male (53%) and 35 female (47%). There were 35 right and 49 left elbows. There were 81 extension-type injuries and three flexion injuries. There were 16 type II and 68 type III fractures. Five cases had extensive soft-tissue swelling. Three children (3.5%) had a pulsless arm initially after trauma. Nine out of 84 (10.7%) had neurological deficits initially after trauma. The mean follow-up was 18.9 months (range 15–24 months).
Surgical technique
The patients are placed in a prone position. A tourniquet is applied but inflated only in cases of open reduction. There must be space for the image intensifier in the AP and lateral views. The first reduction manoeuvre is performed with traction applied to the forearm. The assistant applies countertraction at the shoulder. The translation of the fracture is first reduced. Possible rotational displacements are then corrected with pronation and supination of the forearm. Finally, the shaft-condylar angle is restored by hyperflexing the elbow. Vascular compromise has to be avoided and is controlled by palpating the pulse. During the flexion manoeuvre, pressure is applied to the olecranon to correct for the loss of the shaft-condylar angle.
We prefer to rotate the C-arm during the reduction procedure and subsequent evaluation of the fragments in all views. If the arm is rotated under the C-arm, there is the risk of a loss of the reduction. After the successful reduction manoeuvre, the pulse and capillary perfusion of the hand are evaluated. If vascular compromise is suspected, a Doppler ultrasound is performed.
The most common pattern for crossed pin fixation is having one starting medially and the other starting laterally (Fig. 1a). However, stabilization of the fracture in our cases was achieved by the introduction of two lateral 1.4–1.6 mm Kirschner wires. The first pin was introduced starting from the lateral condyle in a retrograde direction (ascending) to advance to cross the fracture site until it perforates the contra-lateral cortex by 1 or 2 mm. The second pin was introduced in an antegrade (descending) direction from a lateral approach, starting proximal to the fracture line and advancing it across the fracture site into the medial condyle. The ascending pin should perforate the cortex. The descending pin should not perforate the medial condyle more then 1–2 mm (Fig. 1b). This is verified by flouroscopy. The adequacy of the reduction is evaluated with the C-arm in the AP view. For the lateral view, the C-arm is rotated rather than rotating the elbow. The pins are bent 90° and cut with pliers and buried under the skin as close to the bone as possible. The standard is to insert two lateral crossed pins (Fig. 2b). In the case of insufficient stability, a second ascending pin is then introduced.
Fig. 1.
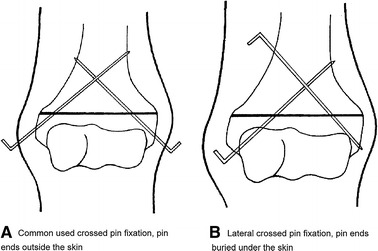
Pin configuration stabilizing supracondylar humerus fractures. a Commonly used crossed pin fixation, pin ends outside the skin. b Lateral crossed pin fixation, pin ends buried under the skin
Fig. 2.

a Anteroposterior of a type III fracture before operation. b Intraoperative radiograph after closed reduction and lateral crossed pin fixation with two K-wires. K-wires buried under the skin. cThe healed fracture after pin removal
In the case of a failed closed reduction, an open reduction is immediately performed by a posterior triceps split approach. The pins are inserted in a medial/lateral cross-pinning technique after identifying the ulnar nerve.
Postoperative immobilization after a closed or open reduction was achieved by applying a long arm cast in 90° of flexion. Immobilization was maintained for four weeks, with a cast change and wound inspection after two weeks. Physiotherapy was only necessary in cases of neurological problems.
The pins were removed after eight weeks with closed pinning and after 3–4 months with open pinning with full anesthesia.
All children responding to the request for return were examined by the primary author. A full examination including functional and cosmetic documentation was performed on each patient. The results were evaluated using Flynn’s clinical and cosmetic functional criteria [14].
In most cases the radiographs present at the time of pin removal were felt to be adequate for analysis. In children where a cosmetic or functional deficit was obvious, new radiographs were taken at the final follow-up examination.
The radiographic evaluations allowed the measuring of the shaft-condylar angle in the lateral views. Any cubitus valgus or varus angulation was measured from the AP view.
Results
Between January 2001 and December 2002 we treated 84 supracondylar fractures with invasive surgical procedure. The results were separated into one of three major categories: (1) radiographic, (2) functional, and (3) cosmetic.
During this two-year period, prompt surgical treatment was always available. Of the 84 children that were treated surgically, 82 had surgery on the day of the injury. Two had a delay of one day, for one closed and one open reduction.
In all, 84 children and their families were sent inquiries by the primary author.
Seventy-five (89%) presented for a clinical and photographic evaluation.
Nine children (11%) could not be contacted and were lost for follow-up.
The mean hospital stay in the group of closed reduction was 2.2 days (range 1–4 days). In the group of open reduction the mean hospital stay was 6.0 days (range 5–9 days).
Radiographic results
In 73 of these 84 patients (87%), the humeral shaft-condylar angle was felt to be normal, ranging between 30° and 40°. Nine of the children (11%), however, had an angle of less than 30°. There was an angle of greater than 40° in two children (2%).
Four of the nine patients with a diminished shaft-condylar angle had a loss of flexion of between 10° and 30°. One patient with an increased shaft-condylar angle had an extension deficit of 20°.
There were no cases of secondary displacement. The nine patients with a humeral shaft angle of less than 30° had a bad initial reduction.
Functional results
The functional results of 75 patients with type II and III were evaluated using Flynn’s score [3]. The results are listed in Table 1.
Table 1.
Functional results
| Reduction | Functional results (Flynn’s score) | |||
|---|---|---|---|---|
| Excellent | Good | Fair | Unsatisfactory | |
| Closed reduction | 42 | 13 | 1 | 3 |
| Secondary open reduction | 7 | 3 | 0 | 1 |
| Immediate open reduction | 3 | 1 | 0 | 1 |
Following closed reduction
From the 59 patients out of 65, 42 had an excellent result, 13 had a good result. One child had a fair result. Two of the three children with an unsatisfactory result had an uncorrected shaft-condylar angle. The Roger’s line (anterior humeral line) passed anterior to the capitellum. In another case, heterotopic ossification, which was visualized anterior to the well-reduced condyle, appeared to contribute to the loss of elbow flexion.
Following open reduction
From the 11 children out of 13 initially treated by secondary open reduction seven had an excellent, three had a good and one had an unsatisfactory result.
From the five children out of six treated with immediate open reduction three had an excellent, one had a good and one had an unsatisfactory result. Following an open reduction, one case had a loss of the shaft-condylar angle, leading to a flexion deficit. One flexion fracture had an increased shaft-condylar angle, which resulted in an extension deficit of 20°.
Cosmetic result
Using Flynn’s score, the cosmetic results were better than the functional results. One child treated by open reduction had developed a cubitus varus of 10°, which needed no further treatment. Eight cases had an increased valgus compared to the healthy side of between 2° and 10°. This did not arouse any concern as to cosmesis on the part of the patients’ parents. The results are listed in Table 2.
Table 2.
Cosmetic results
| Reduction | Cosmetic results (Flynn’s score) | |||
|---|---|---|---|---|
| Excellent | Good | Fair | Unsatisfactory | |
| Closed reduction | 55 | 4 | 0 | 0 |
| Secondary open reduction | 10 | 1 | 0 | 0 |
| Immediate open reduction | 3 | 1 | 0 | 1 |
Treatment by closed reduction
A total of 55 out of 65 children had an excellent result; four had a good result. There were no patients in the group of closed reduction who developed a cubitus varus.
Treatment by open reduction
Ten out of 11 children treated with an open reduction following a failed closed reduction had an excellent cosmetic result and one had a good result. Two children out of the six treated who underwent an immediate open reduction had excellent results. Of the other two re-examined children with immediate open reduction, one had a good result. However, the remaining patient had an unsatisfactory result due to resultant cubitus varus of 10°.
Problems and complications
Common problems and complications occurring following the treatment of displaced supracondylar fractures can be categorized into four major areas:
Infections
Neurological lesions
Vascular problems
Residual angular malalignment.
Each of these areas of complications will be discussed in the following section.
Pin problems
In seven cases of closed reduction we encountered pin migration and penetration through the skin, requiring early removal of one or both pins. Two cases required a short-term antibiotic treatment for superficial pin infections. There were no deep pin infections in any of the cases treated by either a closed or an open reduction.
Neurological lesions
Nine (10.7%) of the children treated with displaced supracondylar fractures had some neurological deficits. The neurological lesions occurred only in patients with type III fractures. These neurological deficits as a result of trauma around the distal humerus disappeared completely within six months, with the exception of one child who complained about a persisting sensory deficit in the area of the median nerve six months following the initial injury.
Vascular problems
Three of the 84 patients presented with a pulseless forearm and hand following an initial injury. In two of these the pulse was restored following a closed reduction of the fracture. In the third child, the pulselessness persisted after a satisfactory closed reduction and pinning of the fracture. While the arm was not pale, it was cooler than the other, thus it was explored surgically by a vascular surgeon who discovered adventitial kinking of the brachial artery. Once this was released the fracture went on to heal with full recovery to produce an excellent result. The only problem was a large scar in the antecubital area of the elbow. Post operatively there was no evidence of any vascular insufficiency.
Residual angular malalignment
In the group treated with an open reduction, one patient had a residual cubitus varus of 10°. In those managed with a closed reduction, eight patients demonstrated minimal valgus malalignment of no greater than 10° compared with the uninjured extremity.
Soft-tissue problems with extensive swelling are possible and common in severe displaced fractures. This is not in itself an indication for an open reduction. In our series there were six children with extensive swelling. In these cases the attending surgeons preferred a primary open reduction.
Discussion
In this day and age, the treatment of displaced supracondylar fractures should be minimally invasive, should have a fair learning curve, and should have a low rate of complications. An outcome close to 80% excellent results, both functional and cosmetic, is to be expected.
While the majority of English-speaking authors are in favor of a closed reduction and percutaneous pin fixation [2, 3, 6, 14], there is one report in the German literature which feels that the optimal anatomic reconstruction of the fracture could be achieved with an open reduction [7]. In our review of the most current literature, it appeared that closed reduction and percutaneous pinning is the treatment of choice in most pediatric trauma centers [2, 3, 4, 5, 6, 15, 16, 17].
In our presented series of 84 displaced fractures, 77% (65) had a successful initial closed reduction. These figures compare favorably to the 60% rate of closed reduction achieved by Millis et al. [18], and 78% by Mazda et al. [4]. One large series from Boston [19] achieved a rate of 92% of initial closed reduction, which was possibly a reflection of their vast experience at that institution. It is our opinion that between 80 and 90% of type III supracondylar fractures should be able to be reduced by a closed method.
In 2003 we achieved an 88.3% (38/43) closed reduction rate. It has been our experience that completely displaced type III supracondylar fractures are easier to reduce than those that are impacted. These latter types of supracondylar fractures tend to have tissue interposition, preventing reduction. Based upon our experience, after analyzing our figures from our institution, it was our policy that closed reduction should always be attempted as the initial treatment. Based upon this past experience, with the exception of six cases, a manipulative closed procedure utilized first has become our protocol to achieve the primary reduction. Following the achievement of an adequate closed reduction, percutaneous pinning is then carried out using two lateral crossed pins with one directed from proximal-lateral to distal-medial. This provided adequate stability. In a discussion of our technique, four points need to be mentioned:
Point 1. Stability studies had demonstrated that crossed pins provided the best stability to counteract rotational stresses. This is also true for the ability to prevent displacement in the varus, valgus, flexion, and extension planes [8, 20]. Other authors, who have used two or three lateral pins, have also found adequate stability in other configurations [2, 8, 21]. Our results are comparable to those of Skaggs et al. [16] whose prospective randomized study found that crossed or parallel wires introduced from a distal to proximal-lateral approach have similar stability.
Point 2. The introduction of the proximal lateral pin is not difficult. The periosteum is typically thick in this age group. So even with an oblique approach the pin easily enters the cortex and can then be advanced toward the medial condyle as it traverses the fracture site.
Point 3. The proximal antegrade pin does not appear to produce an increased risk to the radial nerve. There is a distance of more then 2 cm between the radial nerve in this area on the lateral side and the pin introduction point. In our three cases of radial neuropraxia, which presented initially after the accident and prior to fixation, all disappeared within 2–3 months.
Point 4. The descending pin should not perforate the medial condyle more then 1–2 mm to avoid ulnar nerve injury. This could be verified by flouroscopy when drilling the pin. Ulnar nerve neuropraxia [10, 11, 12, 22] was not encountered in our series at either the initial presentation or after the reduction and pin fixation. This compares to another large series using exclusively a lateral approach but in a different pin configuration [16], which was felt to avoid ulnar nerve damage.
We are in agreement with others [8] that, after closed or open reduction and pin fixation, all of these fractures are best immobilized with a well-padded long arm cast. It has been our policy to leave the patient in the cast for four weeks before mobilization was permitted. With this protocol, we did not see any cases that developed a secondary displacement of the fracture after percutaneous or open pinning with this protocol.
There might be a theoretical risk that the proximal lateral pin can injure the ulnar nerve when drilling through the bony area of the medial condyle. We did not have such a problem in our cases. However, to prevent injury from the proximal lateral pin, we recommend exact flouroscopy-controlled drilling. The pin should end close to the cortex of the medial condyle but not penetrate the cortex.
We recommend burying the pins deep in the skin because of pin infections. Pin infections are described in up to 18% of cases [4]. In a series with lateral cross pinning with proud wires the pin complication rate was 30% [23]. The main problem with the proud pins was excess granulation tissue. In our series even the perforated pins healed after removal without skin problems. The superficial infection rate in our series was 1.2%. The second anaesthesia is a disadvantage, but considering the risk of pin problems we think a second full anaesthesia is justified to eliminate or reduce these concerns.
Between 1 January 2001 and 31 December 2002 we treated 84 patients operatively with supracondylar fractures type II and III. The functional and cosmetic results using Flynn’s score were available in 75 of the children treated. Our 93% good to excellent functional results of all supracondylar fractures treated by closed reduction was comparable to a similar series from France, in which 96% excellent and good results were achieved [4]. Our cosmetic results using Flynn’s score of 93% excellent and 7% good results with no poor results was even better than the French series. A similar series from Kallio et al. [3] achieved 90% excellent or good results, yet 10% were rated as poor.
In some of the older series reported in the 1970s, the success rate was much lower. In one series containing 38 children with displaced fractures undergoing closed pinning, only 76% were found to be acceptable [24]. With the current techniques a success rate of 90% of excellent and good results can be expected. Centers that achieve less than 80% excellent and good results should reassess their protocols and evaluate their need to undergo more training or change their methods of treatment.
Open reduction was achieved in 23% of our cases. The rate of open reduction varies widely in the recent literature. In the 1980s in Kallio’s series [3] 48% needed an open reduction. However, more recently in the 1990s, only 23% in the French series [4] required an open reduction. Our results of cases requiring an open reduction after an attempted closed reduction were similar to those in a more recently published series [4]. We are in disagreement with Scola et al. [7], that an open reduction always produces a superior result. It was our opinion that their conclusion was based upon the experience of several of their cases following a secondary dislocation after an open reduction had been performed in hospitals that apparently had limited experience with this type of fracture.
Conclusion
Most supracondylar fractures should be able to be reduced by closed methods. We are of the opinion that treatment of choice in type II and III fractures is first a closed reduction followed by percutaneous pin stabilization. Crossed pin fixation probably gives the best mechanical stability. We have found that our lateral crossed pinning technique gives excellent stability achieved with crossed pins while having the advantage of avoiding injury to the ulnar nerve.
Acknowledgments
The authors thank Kaye Wilkins for the friendly assistance.
References
- 1.Hasler CC. Supracondylar fractures of the humerus in children. Eur J Trauma. 2001;27:1–15. [Google Scholar]
- 2.Kaewpornsawan K. Comparison between closed reduction with percutaneous pinning and open reduction with pinning in children with totally displaced supracondylar humeral fractures. A randomized controlled trial. J Pediatr Orthop B. 2001;10:131–137. [PubMed] [Google Scholar]
- 3.Kallio PE, Foster BK, Paterson DC. Difficult supracondylar elbow fractures in children: analysis of percutaneous pinning technique. J Pediatr Orthop. 1992;12:11–15. doi: 10.1097/01241398-199201000-00002. [DOI] [PubMed] [Google Scholar]
- 4.Mazda K, Boggione C, Fitoussi F, Pennecot GF. Systematic pinning of displaced extension-type supracondylar fractures of the humerus in children. A prospective study of 116 consecutive patients. J Bone Joint Surg Br. 2001;83:888–893. doi: 10.1302/0301-620X.83B6.11544. [DOI] [PubMed] [Google Scholar]
- 5.Mehserle WL, Meehan PL. Treatment of the displaced supracondylar fracture of the humerus (type III) with closed reduction and percutaneous cross-pin fixation. J Pediatr Orthop. 1991;11:705–711. doi: 10.1097/01241398-199111000-00001. [DOI] [PubMed] [Google Scholar]
- 6.Wilkins KE. Supracondylar fractures: What's new? J Pediatr Orthop B. 1997;6:110–116. doi: 10.1097/01202412-199704000-00006. [DOI] [PubMed] [Google Scholar]
- 7.Scola E, Jezussek D, Kerling HP, et al. Die dislozierte supracondyläre Humerusfraktur des Kindes. Unfallchirurg. 2002;105:95–98. doi: 10.1007/s001130100300. [DOI] [PubMed] [Google Scholar]
- 8.Zionts LE, McKellop HA, Hathaway R. Torsional strength of pin configurations used to fix supracondylar fractures of the humerus in children. J Bone Joint Surg Am. 1994;76:253–256. doi: 10.2106/00004623-199402000-00013. [DOI] [PubMed] [Google Scholar]
- 9.Lyons JP, Ashley E, Hoffer MM. Ulnar nerve palsies after percutaneous cross-pinning of supracondylar fractures in children's elbows. J Pediatr Orthop. 1998;18:43–45. [PubMed] [Google Scholar]
- 10.Rasool MN. Ulnar nerve injury after K-wire fixation of supracondylar humerus fractures in children. J Pediatr Orthop. 1998;18:686–690. doi: 10.1097/01241398-199809000-00027. [DOI] [PubMed] [Google Scholar]
- 11.Royce RO, Dutkowsky JP, Kasser JR, et al. Neurologic complications after K-wire fixation of supracondylar humerus fractures in children. J Pediatr Orthop. 1991;11:191–194. doi: 10.1097/01241398-199103000-00010. [DOI] [PubMed] [Google Scholar]
- 12.Taniguchi Y, Matsuzaki K, Tamaki T. Iatrogenic ulnar nerve injury after percutaneous cross-pinning of supracondylar fracture in a child. J Shoulder Elbow Surg. 2000;9:160–162. doi: 10.1067/mse.2000.103657. [DOI] [PubMed] [Google Scholar]
- 13.Gartland JJ. Management of supracondylar fractures of the humerus in children. Surg Gynecol Obstet. 1959;109:145–154. [PubMed] [Google Scholar]
- 14.Flynn JC, Matthews JG, Benoit RL. Blind pinning of displaced supracondylar fractures of the humerus in children. Sixteen years experience with long-term follow up. J Bone Joint Surg Am. 1974;56:263–72. [PubMed] [Google Scholar]
- 15.Peters CL, Scott SM, Stevens PM. Closed reduction and percutaneous pinning of displaced supracondylar humerus fractures in children: description of a new closed reduction technique for fractures with brachialis muscle entrapment. J Orthop Trauma. 1995;9:430–434. doi: 10.1097/00005131-199505000-00012. [DOI] [PubMed] [Google Scholar]
- 16.Skaggs DL, Hale JM, Bassett J, et al. Operative treatment of supracondylar fractures of the humerus in children. The consequence of pin placement. J Bone Joint Surg Am. 2001;83:735–740. [PubMed] [Google Scholar]
- 17.Topping RE, Blanco JS, Davis TJ. Clinical evaluation of crossed-pin versus lateral-pin fixation in displaced supracondylar humerus fracture. J Pediatr Orthop. 1995;15:435–439. doi: 10.1097/01241398-199507000-00004. [DOI] [PubMed] [Google Scholar]
- 18.Millis MB, Singer IJ, Hall JE. Supracondylar fracture of the humerus in children. Further experience with a study in orthopaedic decision-making. Clin Orthop. 1984;188:90–97. [PubMed] [Google Scholar]
- 19.Reitmann RD, Waters P, Millis M. Open reduction and internal fixation for supracondylar humerus fractures in children. J Pediatr Orthop. 2001;21:157–161. [PubMed] [Google Scholar]
- 20.Kumar R, Malhorta R. Medial approach for operative treatment widely displaced supracondylar fractures of the humerus in children. J Orthop Surg. 2000;8:13–18. doi: 10.1177/230949900000800204. [DOI] [PubMed] [Google Scholar]
- 21.Gordon JE, Patton CM, Luhmann SJ, Bassett GS, Schoenecker PL. Fracture stability after pinning of displaced supracondylar distal humerus fracture in children. J Pediatr Orthop. 2001;21:313–318. [PubMed] [Google Scholar]
- 22.Lee SS, Mahar AT, Miesen D, Newton PO. Displaced pediatric supracondylar humerus fractures: biomechanical analysis of percutaneous pinning techniques. J Pediatr Orthop. 2002;22:440–443. [PubMed] [Google Scholar]
- 23.Shannon FJ, Mohan P, Chacko J, D’Souza LG. Dorgan’s percutaneous lateral cross-wiring of supracondylar fractures of the humerus in children. J Pediatr Orthop. 2004;24:376–379. doi: 10.1097/01241398-200407000-00006. [DOI] [PubMed] [Google Scholar]
- 24.Nacht JL, Ecker ML, Chung SM, et al. Supracondylar fractures of the humerus in children treated by closed reduction and percutaneous pinning. Clin Orthop. 1983;177:203–209. [PubMed] [Google Scholar]