

Summary
The term extranasopharyngeal angiofibroma has been applied to vascular, fibrous nodules occurring outside the nasopharynx. The maxillary sinus is the most common site involved, while the nasal septum represents an extremely rare localization. Computerized tomography scan and magnetic resonance imaging are used to determine the tumour site and its extension. Surgical excision of the mass is the treatment of choice, and recurrence is rare. Typically, clinical characteristics of extranasopharyngeal angiofibromas do not conform with that of nasopharyngeal angiofibromas and, for this reason, these tumours must be regarded as a separate entity. Due to these different features, extranasopharyngeal angiofibromas can present a diagnostic challenge and a meticulous evaluation with a high index of suspicion is essential in establishing the correct diagnosis and treatment. We report the case of a 57-year-old female with a 1-year history of a slowly progressing right nasal obstruction due to the presence of a whitish mass adhering to the posterior nasal septum. The patient was succesfully treated surgically. Histopathological findings were compatible with a diagnosis of angiofibroma. Extranasopharyngeal angiofibroma must be taken into consideration in the differential diagnosis of nasal vascular tumours and nasal septum should be regarded as a potential, though exceptional, localization of these neoplasms.
Keywords: Nose, Benign tumours, Nasal septum, Angiofibroma, Extranasopharyngeal angiofibroma
Riassunto
Con il termine angiofibroma extrarinofaringeo si intende denominare una lesione di tipo fibrovascolare che origina al di fuori del cavo rinofaringeo. Il seno mascellare è la sede più comunemente interessata, mentre il setto nasale rappresenta una localizzazione estremamente rara di questa neoplasia. La tomografia computerizzata e la risonanza magnetica sono le indagini utilizzate per determinare la sede e l’estensione di queste neoformazioni. Tipicamente, le caratteristiche cliniche dell’angiofibroma extrarinofaringeo non rispecchiano quelle dell’angiofibroma a origine rinofaringea e, per tale motivo, questa lesione deve essere considerata una entità a sé stante. A causa di queste differenti caratteristiche, la neoplasia può rappresentare una sfida in termini diagnostici; pertanto, una valutazione metodica della lesione è essenziale ai fini di un corretto inquadramento diagnostico e terapeutico. Riportiamo il caso di una paziente, di 57 anni, con una storia clinica di ostruzione respiratoria nasale, insorta gradualmente nel corso dell’ultimo anno a causa di una massa biancastra aderente al setto nasale posteriormente. La paziente è stata trattata chirurgicamente con successo. Il riscontro istopatologico è risultato compatibile con la diagnosi di angiofibroma. L’angiofibroma extrarinofaringeo deve essere preso in considerazione nella diagnosi differenziale dei tumori vascolari del naso e il setto nasale deve essere ritenuto una localizzazione possibile, seppur rara, di queste neoplasie.
Introduction
In 1980, De Vincentiis and Pinelli 1 reviewed a series of 704 cases of angiofibroma and found that 13 cases manifested outside the nasopharynx, thus suggesting that extranasopharyngeal localization of this tumour is a possible, although rare occurrence. Since then, numerous studies have reported cases of angiofibroma localized in unusual sites 2–5. A recent review of the literature reported a total of 65 patients with atypical localizations of nasopharyngeal angiofibromas 6, the maxillary sinus being the most commonly involved site 4. Nasal septum represents an extremely rare localization with only 6 cases having been reported in the international literature to date 4 6 7. Besides the different location, typical clinical characteristics of extranasopharyngeal angiofibromas, such as, symptoms, age, sex, do not conform to a great extent with that of nasopharyngeal angiofibromas. This fact has led to doubt as to whether extranasopharyngeal angiofibromas, though structurally similar, should be considered as being different from nasopharyngeal angiofibroma 8. Recently, Celik et al. 9 also proposed that patients, who have different characteristics other than the classical angiofibromas, should be referred to as “atypical angiofibroma”. Due to these different features, extranasopharyngeal angiofibromas can present a diagnostic challenge and a meticulous evaluation with a high index of suspicion is essential in establishing the correct diagnosis and treatment. Herein, a rare case is reported of angiofibroma originating from the nasal septum and the idea is, therefore, supported that extranasopharyngeal angiofibromas must be regarded as a separate entity.
Case report
A 57-year-old female presented at the Otolaryngology Department of Imola Hospital with a one-year history of a slowly progressing right nasal obstruction. The patient had no previous history of trauma or infection. On ENT examination, anterior rhinoscopy showed a nasal septum deviation on the right side, while nasal endoscopy revealed a whitish mass adhering to the posterior septum and filling the right choana. A contrast enhanced computerized tomography (CT) scan of the skull showed a mild contrast enhancing mass arising from the vomerian nasal septum and extending backwards within the right choana (Fig. 1 A, B). There was no extension beyond the nasal cavity into the nasopharynx or any paranasal sinuses. After performing septoplasty, the mass was probed by a sucker. It presented of hard consistency, minimally bleeding, and firmly adhering to the bony nasal septum. Thereafter, the tumour was elevated with the underlying periosteum and removed en bloc under endoscopic guidance. A biopsy specimen of the mass 3-4 cm in diameter was obtained (Fig. 2). Intra-operative bleeding was minimal. A soft anterior nasal pack was placed bilaterally. Post-operative recovery was uneventful. The pack was removed after 48 hours and the patient was discharged without any complications. Histopathological examination revealed dilated, cavernous vascular spaces lined with endothelial cells and separated by fibrostroma with stromal cell nuclei. These findings were compatible with a diagnosis of angiofibroma (Fig. 3). At one-year follow-up, nasal endoscopy showed a well-aligned septum with no evidence of residual or recurrent disease.
Fig. 1.

CT scan of the skull showing a mass arising from vomerian nasal septum and extending backwards within right choana (A: coronal view; B: axial view).
Fig. 2.

Excisional biopsy specimen of a whitish mass measuring 3-4 cm in diameter.
Fig. 3.
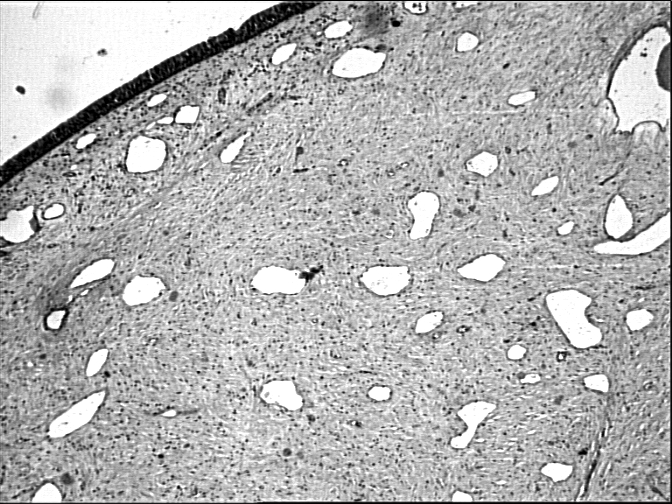
Histopathology of angiofibroma composed of fibrous connective tissue interspersed with endothelium-lined vascular spaces.
Discussion
Nasopharyngeal angiofibroma is a well-defined entity sharply localized in time, space, and sex. The tumour virtually always arises from the nasopharynx and only later may extend into the nasal cavity 10. More recently, the term extranasopharyngeal angiofibroma has been applied to vascular, fibrous nodules occurring outside the nasopharynx. However, extranasopharyngeal angiofibroma have virtually nothing in common with nasopharyngeal tumours and the use of the term angiofibroma for these lesions may therefore be confusing. In fact, these rare, benign, neoplasms are characterized by a different biological history and clinical features with respect to nasophayngeal tumours and, for these reasons, they should be regarded as a separate clinical entity. Compared to nasopharyngeal angiofibromas, patients affected are older, females can also be involved, symptoms develop more quickly, and hypervascularity is less common 5. The case described here fulfilled all these features. The clinical presentation of extranasopharyngeal angiofibroma depends mainly on the localization and extent of the tumour. In those cases arising from nasal cavities, nasal obstruction and epistaxis are the more frequently reported symptoms. As far as concerns instrumental diagnosis, CT scan and magnetic resonance imaging (MRI) are used to determine the tumour site and its extension, with special attention being focused on skull base involvement, intracranial spread and relationship to important vascular and neurologic structures 11. While bone erosion can be more easily rervealed by CT scan, MRI is adequate in demonstrating cortical erosion and cancellous replacement by tumour. The administration of a contrast agent in nasopharyngeal angiofibroma leads to a strong and usually homogeneous enhancement on CT and MRI T1 sequences 12. On the other hand, extranasopharyngeal angiofibroma usually enhances contrast medium or even nothing, due to the frequent poor vascularity of the tumour 10. Alvi et al. 3 consider CT scan to be sufficient for the diagnosis of extranasopharyngeal angiofibroma, as it clearly delineates and identifies the tumour. However, signs of suspected hypervascularity, upon CT scan or MRI, indicate the need for arteriography prior to surgical procedures in order to arrange the necessary precautions, such as embolization, and reduce the risk of brisk bleeding during biopsy or tumour removal. In this case, the poor vascularity of the lesion did not require preoperative embolization. Surgical excision of the mass is the treatment of choice, and recurrence is rare 2. Extranasopharyngeal angiofibroma must be taken into consideration in the differential diagnosis of nasal vascular tumours and the nasal septum should be regarded as a potential, though exceptional, localization of these neoplasms. Clinically, extranasopharyngeal angiofibromas, such as the one described in this case, fall into that category of odd presentations that do not fit within the accepted clinical parameters that one always expects to find in cases of angiofibroma. Whether these lesions represent, in fact, an angiofibroma or a variant of another lesion, is, it would appear, still open to discussion.
References
- 1.De Vincentiis G, Pinelli V. Rhinopharyngeal angiofibroma in the pediatric age group. Clinical-statistical contribution. Int J Pediatr Otorhinolaryngol 1980;2:99-122. [DOI] [PubMed] [Google Scholar]
- 2.Sarpa JR, Novely NJ. Extranasopharyngeal angiofibroma. Otolaryngol Head Neck Surg 1989;101:693-7. [DOI] [PubMed] [Google Scholar]
- 3.Alvi A, Myssiorek D, Fucks A. Extranasopharyngeal angiofibroma. J Otolaryngol 1996;25:346-8. [PubMed] [Google Scholar]
- 4.Huang RY, Damrose EJ, Blackwell KE, Cohen AN, Calcaterra TC. Extranasopharyngeal angiofibroma. Int J Pediatr Otorhinolaryngol 2000;561:59-64. [DOI] [PubMed] [Google Scholar]
- 5.Akbas Y, Anadolu Y. Extranasopharyngeal angiofibroma of the head and neck in women. Am J Otolaryngol 2003;24:413-6. [DOI] [PubMed] [Google Scholar]
- 6.Windfuhr JP, Remmert S. Extranasopharyngeal angiofibroma: etiology, incidence and management. Acta Otolaryngol 2004;124:880-9. [DOI] [PubMed] [Google Scholar]
- 7.Somdas MA, Ketenci I, Unlu Y, Canoz O, Guney E. Extranasopharyngeal angiofibroma originating from the nasal septum. Otolaryngol Head Neck Surg 2005;133:1-2. [DOI] [PubMed] [Google Scholar]
- 8.Lucas RB. Pathology of tumours of the oral tissues. Third Edn. Edinburgh: Churchill Livingstone 1976. [Google Scholar]
- 9.Celik B, Erisen L, Saraydaroglu O, Coskun H. Atypical angiofibromas: a report of four cases. Int J Pediat Otorhinolaryngol 2005;69:415-21. [DOI] [PubMed] [Google Scholar]
- 10.Harrison DF. The natural history, pathogenesis, and treatment of juvenile angiofibroma. Personal experience with 44 patients. Arch Otolaryngol Head Neck Surg 1987;113:936-42. [DOI] [PubMed] [Google Scholar]
- 11.Schick B, Kahle G. Radiological findings in angiofibroma. Acta Radiol 2000;41:585-93. [DOI] [PubMed] [Google Scholar]
- 12.Maroldi R, Berlucchi M, Farina D, Tomenzoli D, Borghesi A, Pianta L. Benign neoplasm and tumor-like lesions. In: Maroldi R, Nicolai P, editors. Imaging in treatment planning for sinonasal diseases. Berlin, Heidelberg, New York: Springer Verlag 2005. p. 107-58. [Google Scholar]