
Figure 2.
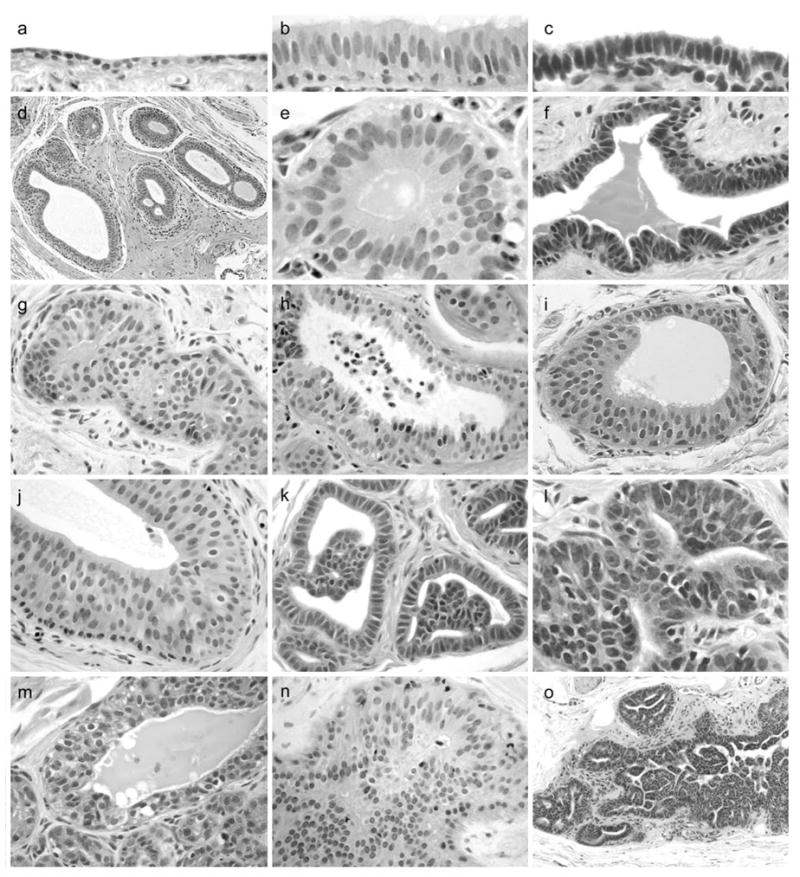
Morphologic features of mammary gland epithelial lesions. (a), normal duct with flattened cuboidal epithelium (left). (b) – (c), columnar cell change (CCC) variants showing luminal cells with ovoid to elongate nuclei aligned perpendicular to the basement membrane. (d), terminal ductal lobular unit (TDLU) with dilation of terminal ducts lined by columnar luminal cells. (e) – (f), CCC variants without atypia. (g), columnar cell hyperplasia (CCH) without atypia showing luminal cells in >2 layers with partial luminal obstruction. (h) CCH with tufting and apical secretory blebs (consistent with human “columnar alteration with prominent secretory snouts,” or CAPSS lesion). (i) – (j) CCH with low-grade monomorphic nuclear atypia and a flat apical surface (consistent with human “flat epithelial atypia,” or FEA lesion). (k) – (l), atypical ductal hyperplasia (ADH) lesions with micropapillary-type architecture. (m), atypical lobular hyperplasia (ALH) showing multiple layers of secretory acinar cells, bordered below by small normal lobuloalveolar acini. (n) – (o), ductal carcinoma in situ (DCIS) lesions with cells arranged in sheets, micropapillae, and fenestrated bridges.