
Figure 11.
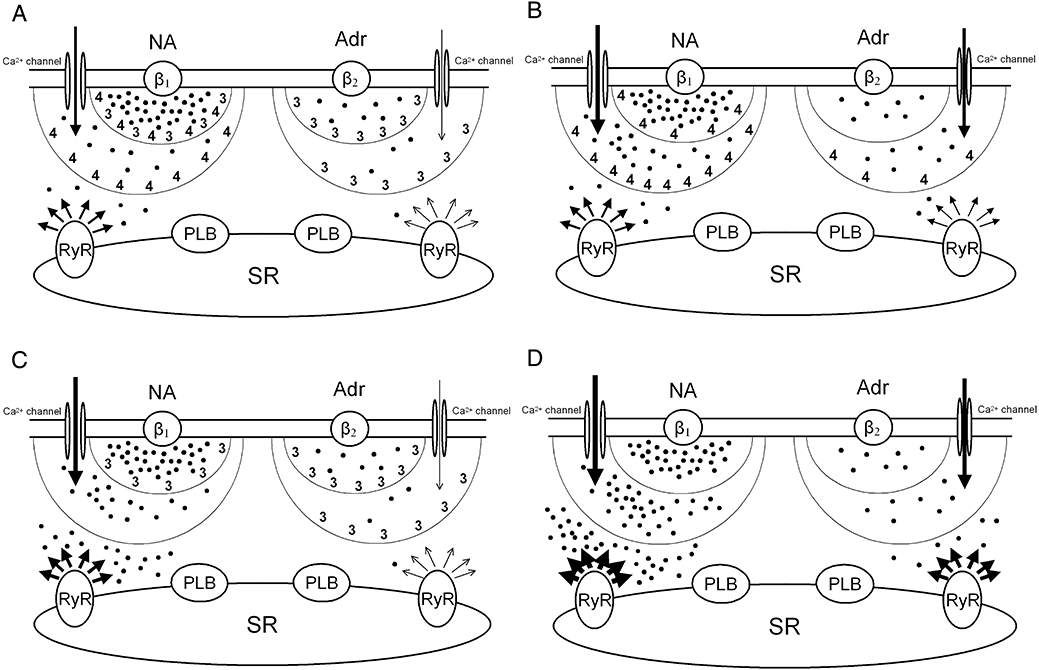
Hypothetical regulation of cAMP levels by activated PDE3 (3) and PDE4 (4) in compartments at different distances from activated β1- and β2-adrenoceptors in rat ventricle. (A) Physiological situation. (B) Inhibition of PDE3. (C) Inhibition of PDE4. (D) Inhibition of both PDE3 and PDE4. Black dots represent steady state concentrations of cAMP in each domain. (−)-Noradrenaline (NA) and (−)-adrenaline (Adr) stimulate β1- and β2-adrenoceptors, respectively, thereby increasing the production of cAMP and activating PDE3 and PDE4. Two sequential barriers, formed by activated PDEs, break down cAMP. The composition of PDEs in both barriers is different for β1- and β2-adrenoceptors. L-type Ca2+ channel function is enhanced by cAMP and only reduced by PDE activity of the first barrier (smaller half-circle), whereas inotropically relevant cAMP has to pass through the more distal second barrier (larger half-circle) to reach the SR. The first barrier corresponds to PDE3 and PDE4 bound to the sarcolemma. The second barrier is produced by PDE3 and PDE in the cytoplasm and at the SR. Arrows represent Ca2+ current through L-type channels and Ca2+ release from RyR2 channels (RyR). Arrow thickness is proportional to ICa-L and Ca2+ release. The inotropic responses are assumed to be proportional to Ca2+ released from the SR through RyR2 channels. The cAMP-dependent activation of PKA and subsequent PKA-catalysed phosphorylation of Ca2+ channels, phospholamban (PLB), PDE4 and RyR2 is not represented to avoid overcrowding. Both PDE3 and PDE4 blunt the ICa-L response to (−)-noradrenaline (NA) mediated through β1-adrenoceptors but only PDE3 blunts the ICa-L response to (−)-adrenaline mediated through β2-adrenoceptors. Positive inotropic responses to both (−)-noradrenaline (β1-adrenoceptors) and (−)-adrenaline (β2-adrenoceptors) are assumed to occur at least in part through PKA-catalysed phosphorylation of Ca2+ channels, RyR2 channels and phospholamban (PLB). The positive inotropic effects of catecholamines are controlled by PDE4 through β1-adrenoceptors but by PDE3 through β2-adrenoceptors.