
Figure 1.
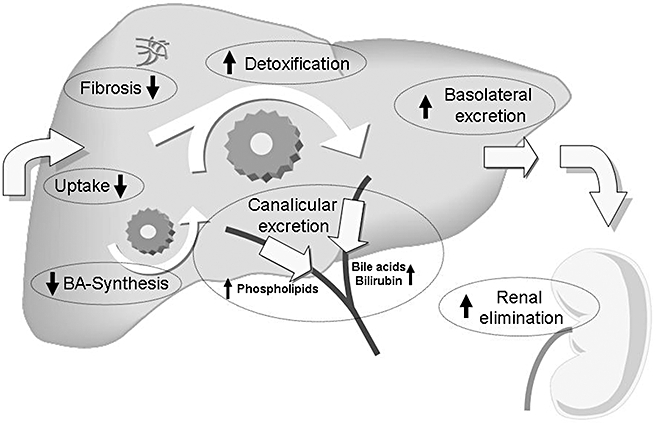
Targets for nuclear receptor ligands in cholestasis. Therapeutic approaches in cholestasis should primarily aim at limiting accumulation of toxic biliary constituents (especially bile acids, BA). This can be achieved by reducing basolateral hepatic uptake and by increasing orthograde canalicular and retrograde (alternative) basolateral secretion. Increasing canalicular secretion will also lead to an increase in bile flow, which might be beneficial in some (early and primarily canalicular) forms of cholestasis. In obstructive cholestasis, however, an increase in bile flow will lead to an increase in biliary pressure with subsequent rupture of cholangioles and liver injury. Stimulating alternative basolateral secretion of water soluble compounds into sinusoidal blood is followed by increased renal elimination of these substances. Increasing water solubility and reducing toxicity can be achieved by phase I and phase II detoxification reactions that also facilitate renal elimination due to reduced albumin binding. In addition, repression of bile acid synthesis will also reduce bile acid accumulation. Other therapeutic strategies in cholestasis include reduction of the toxicity of bile by increasing the biliary phospholipids content and direct inhibition of fibrosis. All these protective mechanisms are regulated to a large extent at a transcriptional level by nuclear receptors. Therapeutic administration of nuclear receptor ligands can activate these defence pathways. Adapted from SJ Karpen, Hepatology 2005 (Karpen, 2005).