
Figure 5.
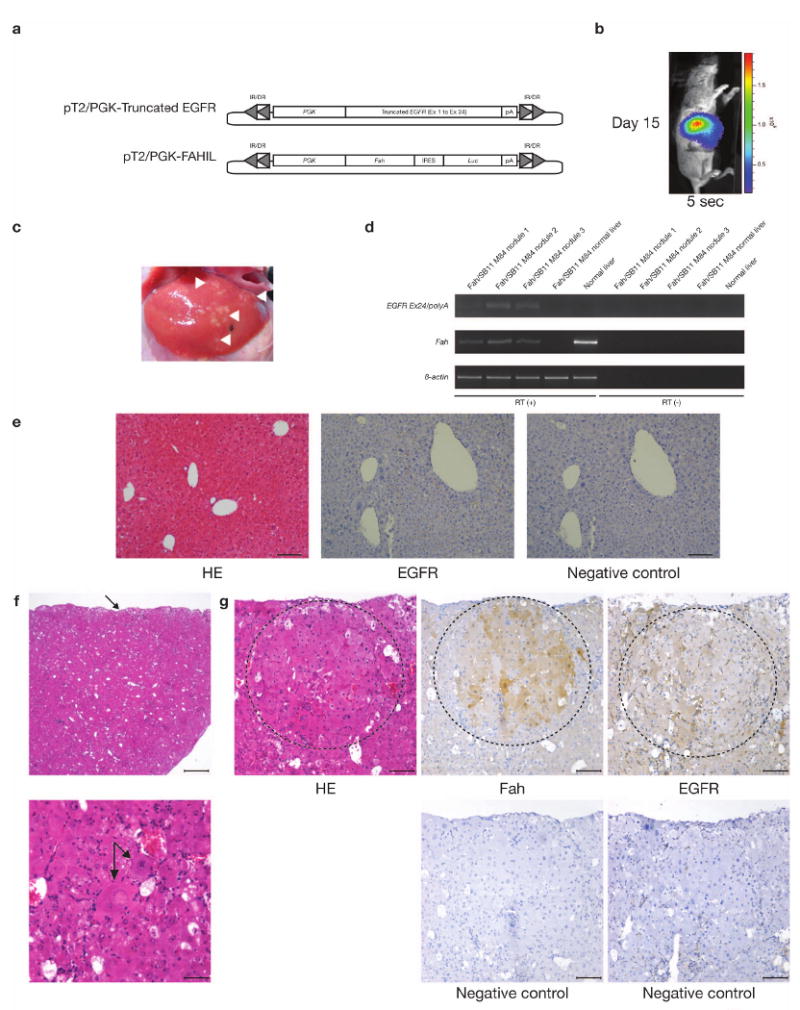
Validating the oncogenic potential of truncated EGFR using the Fumarylacetoacetate hydrolase (Fah)-deficient mouse model. (a) Vectors used for tail vein hydrodynamic injection. pT2/PGK-Truncated EGFR, truncated EGFR cDNA (exon 1 to exon 24) placed under the control of the Phosphoglycerate kinase (PGK) promoter and flanked by SB inverted repeat/direct repeat (IR/DR) recognition sequences essential for transposition. pT2/PGK-FAHIL, Fumaryl acetoacetate hydrolase (Fah) cDNA placed under the control of the PGK promoter fused with an IRES-Luciferase (Luc) reporter gene, flanked by SB IR/DRs. (b) Luciferase activity in Fah/SB11 M84 taken 15-days post-injected with pT2/PGK-Truncated EGFR and pT2/PGK-FAHIL. Exposure time was 5-seconds. (c) Validating the tumorigenic potential of truncated EGFR using the Fah-deficient mouse model. At 43-days post-hydrodynamic injection, Fah/SB11 M84 was killed and the abdominal cavity opened, revealing many patches of small hyperplastic liver nodules (arrowheads). These nodules were carefully removed for RNA extraction and subsequent RT-PCR analyses. Adjacent normal liver tissue was also extracted for comparison. (d) RT-PCR analyses of the liver nodules and adjacent normal tissue. Liver hyperplastic nodules were expressing both Fah and the truncated form of EGFR, while the adjacent normal tissue was negative for both transcripts. RT (+), first strand cDNA synthesis with reverse transcriptase added; RT (−), first strand cDNA synthesis without reverse transcriptase. (e) Normal histology of Fah-deficient liver (hematoxylin-eosin stain, HE) and lack of EGFR detectable by immunohistochemical (IHC) staining. EGFR, treated with EGFR primary antibody; Negative control, serial section not treated with the indicated primary antibody. Scale bars, 100 μm. (f) Histology of liver hyperplastic nodules induced by truncated form of EGFR. Top HE panel, capsular surface of the liver was irregularly nodular (arrow) but overall hepatic architecture was preserved with regularly spaced central veins and portal tracts. Scale bar, 500 μm. Bottom HE panel, a portion of hepatic lobule containing variably sized hepatocytes with 2 cytomegalic and karyomegalic hepatocytes in the center one of which is binucleated (arrows). Occasional hepatocytes have vacuolated cytoplasm. Hepatic cords are not evident due to cellular crowding. Scale bar, 50 μm. (g) Hyperplastic nodule (enclosed within dashed circular line) within hepatic parenchyma consisted of closely packed sheets of variably sized hepatocytes including a karyomegalic cell. Note mild compression of surrounding hepatic parenchyma. There was low degree of inflammation represented by scattered neutrophils and lymphocytes and mild extramedullary hematopoiesis. IHC analyses of serial liver sections treated with the indicated primary antibody confirmed the co-expression of Fah and EGFR in liver nodules. Most of the hepatocytes within hyperplastic nodule (enclosed within dashed circular line) expressed Fah. Hepatocytes within hyperplastic nodule (enclosed within dashed circular line) and within surrounding parenchyma stained weakly for EGFR. EGFR staining is also prominent in the cytoplasmic membranes of cells bordering sinusoids. Negative control, serial sections not treated with the indicated primary antibody. Scale bars, 100 μm.