
Figure 2.
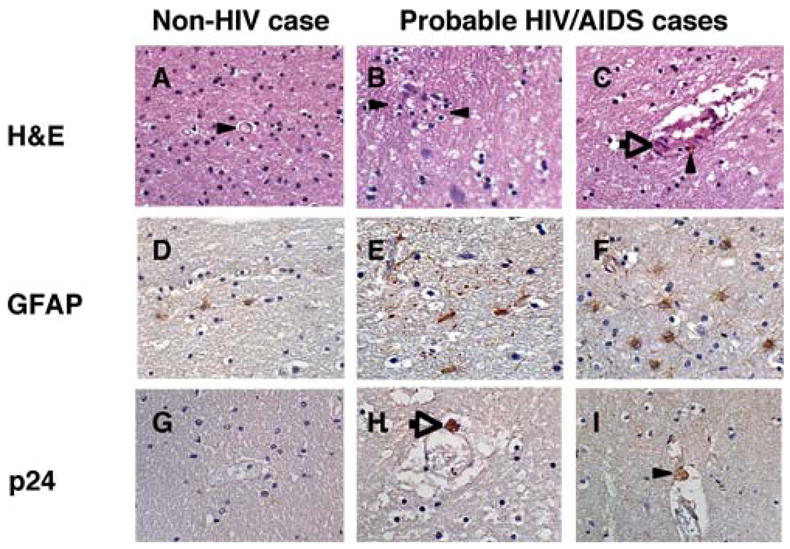
Neuropathological findings in sections from white matter tracts underlying frontal cortex stained with H&E (Panels A–C); anti-GFAP antibody (Panels D–F); or anti-HIV p24 antibody from a subset of autopsy cases from Addis Ababa. Panels A, D, G are sections from a 37-year-old individual who died from a gunshot wound to the abdomen, with no evidence of chronic illness or brain trauma; Panels B, E, H are sections from the case shown in Figure 1. Panels C, F, I are sections from a 55-year-old patient with PTB who died from pneumonia with hepatomegaly and suspected HIV/AIDS. A) H&E stain showing well-preserved white matter and vascular architecture (arrowhead), with no evidence of lymphocytic infiltration; B) H&E stain showing extensive vacuolarization of white matter and microglial nodular formation (arrow); C) H&E stain showing disruption of vascular architecture with white matter vacuolarization, lymphocytic and macrophage infiltration (arrowhead); D) GFAP immunoreactivity observed in a normal control; E) GFAP immunoreactive astrocytes surrounding an area suggestive of a migroglial nodule; F) GFAP immunoreactivity indicating reactive gliosis in a case with accompanying white matter damage; G) Absence of HIV-p24 immunoreactivty in the non-HIV case; H) HIV-p24 immunoreactive macrophage closely abutting capillary (arrow) with accompanying white matter vacuolarization; I) HIV-p24 immunoreactivity in a macrophage closely abutting capillary (arrowhead). H&E: hematoxylin and eosin; GFAP: glial fibrillary acidic protein; p24: HIV p24 protein.