

Abstract
Purpose
This investigation addressed two main questions: (1) How do toddler's spoken utterances change during the first year of Cochlear Implant (CI) use? (2) How do the time-courses for reaching spoken word milestones after implant activation compare with those reported for typically developing children? These questions were explored to increase understanding of early semantic development in children who receive cochlear implants before their second birthdays.
Methods
Monthly recordings of mother-child interactions were gathered during the first year of CI use by a boy and a girl whose cochlear implants were activated at 11 and 21 months of age, respectively. Child utterances were classified as non-words, pre-words, single words, or word combinations and the percentages of these utterance types were calculated for each month. Data were compared to published findings for typically developing children for the number of months of robust hearing (i.e., auditory access to conversational speech) needed to reach spoken word milestones, and the chronological ages at which milestones were achieved.
Results
The main findings were that the percentages of non-words and pre-words decreased as single words and word combinations increased; both children achieved most spoken word milestones with fewer months of robust hearing experience than reported for typically developing children; the youngest recipient achieved more milestones within typical age-ranges than the child implanted later in life.
Conclusions
The children's expeditious gains in spoken word development appeared to be facilitated by interactions among their pre-implant hearing experiences, their relatively advanced physical, cognitive, and social maturity, participation in intervention programs, and the introduction of robust hearing within the Utterance Acquisition phase of language development as proposed in the Neurolingusitic theory (Locke, 1997).
Keywords: Spoken Word Development, Cochlear Implants, Age at Implantation
The implementation of newborn hearing screening and decreases in age criterion for cochlear implantation have made it possible for many children who are deaf to experience greatly improved hearing sensitivity during the first 2 years of life. Very young cochlear implant (CI) recipients provide a unique opportunity to examine the impact of increased access to conversational speech on the initial phases of spoken language development. This investigation examined changes in the types of spoken utterances produced, and the time-courses for attaining spoken word milestones during the first year of CI experience for two such children. Descriptions of these phenomena are needed to increase understanding of the nature of CI-assisted language learning following a period of very limited auditory sensitivity, to bolster efforts to identify an optimal age-range for cochlear implantation surgery, and to inform intervention practices for very young CI recipients.
Typical Patterns and Rates of Spoken Word Development
Infants who are typically developing show predictable changes in their vocal behaviors during the first two years of life (Nathani, Ertmer, & Stark, 2006; see Vihman, 1996 for review). Their utterances progress from those that are not very speech-like (e.g., grunts and squeals and vowels in isolation), to more adult-like combinations of consonants and vowels that carry no apparent meaning (e.g., canonical babbling; Oller, 1980; Stark, 1980), to attempts to communicate that are not recognizable as words (e.g., pre-words; Fletcher & Garman, 1979), to utterances that contain enough of the phonetic characteristics of adult models to be recognized as words, and finally--around two years of age--to word combinations. Whereas speech development during the first year of life is characterized by segmental and suprasegmental advances within the context of non-meaningful utterances, the second year of life is most noteworthy for the emergence of spoken words. The nature of pre-linguistic speech development in young CI recipients is receiving increasing research attention (e.g., Ertmer, Young, & Nathani, 2007; Moore & Bass-Ringdahl, 2002; Schauwers, Gillis, Daemers, de Beuklaer, & Govaerts, 2004). Currently, however, little is known about how children who are deaf progress from mainly non-meaningful utterances and pre-words, to the abundant production of recognizable words and word combinations after CI activation. Data from children who are typically developing can provide a general basis for assessing the time-course and describing the characteristics of this transitional period.
Spoken words are among the most widely anticipated and readily observable indicators of language acquisition in typically developing infants and toddlers (Fenson, Dale, Resnick, & Bates, 1993). Identifying the ages at which children typically reach spoken word milestones has long been a major focus of research in the field of child language development (see Bates, O'Connell, & Shore, 1987; Ingram, 1989 for reviews). Researchers have relied on parental diary accounts, direct observation of parent-child interactions, and parent checklists to estimate children's rate of word learning. Although criteria for identifying spoken words have varied across studies, several age-based milestones have been established by observing parent-child interactions when children were between 10 and 24 months of age. The findings of observational studies are highlighted next because the current study used this approach.
Observational studies have shown that children's first words typically emerge between 10 and 13 months (Bates, et al., 1987; Snyder, Bates, & Bretherton, 1981), that children produce approximately four words during 30-minute interactions by 11- 12 months, and 25 words by 16 months (deBoysson-Bardies et al., 1992). Children also reduce the production of prelinguistic utterances (non-words) as words emerge, reaching a 1:1 ratio between single words and non-words by 13 - 21 months of age. This ratio doubles to 2:1 shortly thereafter (Robb, Bauer, & Tyler, 1994). The emergence of word combinations (18 – 24 months) signals the end of the single-word period (Bates, et al., 1987). In general, data from parent reports overlap with these observational findings. For example, they show first words emerging between 8 – 16 months (Fenson et al., 1993), and 10 words by 11 – 15 months (Vihman & Miller, 1988), and word combinations around 24 months (Ingram, 1989).
In addition to providing some of the spoken word milestones cited above, Robb et al., (1994) sought to determine whether the single-word stage (defined as the period when the first 50 different words are produced) represented a discrete shift to meaningful speech or whether it could be more accurately characterized as a continuum in which non-words co-occurred with single word productions. After observing six children who were typically developing (ages 8 – 14 months at the start of the study) for 1 year, the authors determined that non-words persisted throughout the single-word stage, and concluded that single-word stage represented an increase in speech intelligibility more so than a discrete developmental period. It remains to be seen how closely this characterization and other spoken word milestones apply to young CI recipients.
Spoken Language Gains in Children with Cochlear Implants
Advances in multi-channel cochlear implant technology have enabled children who are deaf to have greatly increased access to conversational speech (ASHA technical report, 2004). Improved access to ambient speech models has resulted in substantial increases in speech perception, speech production, and language abilities for preschool and school-age children (e.g., Bollard, Chute, Popp, & Parisier, 1999; Chin, Tsai, & Gao, 2003; Fryhauf-Bertschy, Tyler, Kelsay, Gantz, & Woodworth, 1997; Geers, Brenner, & Davidson, 2003). Researchers have also found that greater communication gains can be expected when children are implanted at progressively younger ages (e.g., Connor, Hieber, Arts, & Zwolan, 2000; Miyamoto, Kirk, Svirsky, & Sehgal, 1999; Nikolopoulos, O'Donoghue, & Archbold, 1999; Tomblin, Barker, Spencer, Zhang, & Gantz, 2005).
Recent research supports the efficacy of cochlear implantation in infants and toddlers. In an analysis of language outcomes for 29 children who were implanted between 10 and 40 months, Tomblin and colleagues (Tomblin et al., 2005) found that “children implanted earlier in life reached higher levels of expressive language proficiency than the children implanted later in life, despite being at least 3 years younger” (p. 862-63). Similarly, Spencer (2004) found that younger ages of implantation (range: 14 – 27 months) were associated with higher language scores. A report by Connor, Craig, Raudenbush, Heavner, and Zwolan (2006) identified “added value” (p. 628) for earlier implantation in children who are oral communicators, noting that those implanted before 2;6 exhibited early bursts of growth in consonant-production accuracy and vocabulary compared to those who received CIs later in life. These studies were conducted after the children had between 1 and 13 years of CI use. Researchers have also begun to examine speech and language development during the first year of CI use.
Early Speech and Language Development in Young Cochlear Implant Recipients
Pre-linguistic vocal development is the process by which infants and toddlers “produce increasingly complex, phonetically diverse, and speech-like utterances before they say words on a regular basis” (Ertmer, 2005, p.85). A recent study of vocal development in young CI recipients found that higher levels of development were achieved with “fewer months of hearing experience than observed for typically developing infants” (Ertmer et al., 2007, p. 393) by six of seven children who were implanted by 3;0 (Note: the remaining child was identified as having multiple disabilities). Rapid progress in vocal development has also been documented in other young CI recipients (e.g., Ertmer & Mellon, 2001; McCaffrey, Davis, MacNeilage, & von Hapsburg, 1999; Moore & Bass-Ringdahl, 2002; Schauwers, Gillis, Daemers, de Beuklaer, & Govaerts, 2004). The consistency of these findings raises the possibility that advancements in spoken word production might also be accelerated. Two case studies have examined this possibility in a single young CI recipient.
“Hannah” was implanted at 19 months and was reported by her mother to understand almost 240 words and say approximately 90 words after 12 months of implant experience (Ertmer & Mellon, 2001). Thus, the size of her spoken word vocabulary after 1 year of CI use was far greater than expected for year-old infants who are typically developing. A follow-up study of the same child (Ertmer, Strong, & Sadagopan, 2003) examined 30-minute mother-child interactions that were video-recorded at 6-month intervals between the 13th and 42nd month of implant experience. The main findings were (1) at the start of the study (i.e., after13 months of CI experience), Hannah produced approximately one word or word combination for every three non-word utterances, (2) a 1:1 word to non-word ratio was first observed after 17 months of CI use, and (3) a 2:1 word to non-word ratio was first observed in month 20. The authors concluded that, for Hannah, cochlear implantation at a young age, in combination with intact biological, cognitive, and social systems, and participation in aural habilitation programs, appeared to facilitate an early spurt of word learning and a near-typical time-course for achieving the word : non-word ratios identified by Robb et al., (1994). Further consideration requires that pre-implantation hearing experiences also be acknowledged as potential contributors to early language learning.
Auditory Access to Speech: When Does it Begin?
Pediatric candidates for cochlear implantation are required to participate in a trial period with hearing aids to determine whether implant surgery is warranted. It is important to recognize that children may gain some access to speech models and auditory feedback during this trial and that these experiences may contribute to later gains in spoken language development. For instance, children with some low to mid-frequency residual hearing may detect fundamental frequency information, some formant information for vowels, and speech timing and intensity cues, via amplification. These pre-CI auditory experiences may be helpful for developing spoken language once an implant is received (Szagun, 2001). When children exhibit very limited responses to sounds and speech during the hearing aid trial, however, spoken language development is likely to be delayed substantially if amplification remains the sole means of accessing auditory information (see Carney & Moeller, 1998 for review). For children who subsequently receive CIs, increased access to a wide range of speech cues is likely to be a major contributor to spoken language development, along with benefits from prior hearing experiences with hearing aids, participation in intervention, and within-child learning abilities (Geers, 2002).
The term “robust hearing” will be used in this report to indicate auditory access to speech at conversational intensity levels (i.e., mean of approximately 65 dB SPL / 45 dB HL across 250 – 8000 Hz; Fletcher, 1953). For children with CIs, the number of months of robust hearing is considered equivalent to the amount of CI experience they have. For children who are typically developing, months of robust hearing is equivalent to chronological age (CA). For the purposes of the current report, months of robust hearing experience will be used to compare the time-courses for reaching spoken word milestones in these two groups of children. Several general outcomes are possible from this comparison.
Possible Spoken Word Outcomes in Young Children with Cochlear Implants
Children who receive CIs by their second birthday begin to experience robust hearing within an age-range when much semantic knowledge is typically acquired. At least three outcomes seem possible as these children begin to say spoken words. First, young CI recipients might require typical amounts of robust hearing experience to reach spoken word milestones. For example, they might require at least 10 months of robust hearing before saying their first words--as seen in typically developing children. This would suggest that spoken word development is strongly influenced by the amount of robust hearing children experience. If observed widely, a typical rate of development after implantation would seem to suggest that a period of auditory deprivation has a negative impact on spoken language development because the gap between young CI users and their typical age-peers would continue to increase during the first year of implant experience. The improvements documented for pediatric CI users in general (ASHA, 2004), and the relatively greater gains of children implanted at younger versus older ages (e.g., Conner et al., 2006) suggest that this outcome would be unlikely for toddlers who participate in communication intervention and have no impediments to language acquisition besides hearing loss.
A second possible outcome is that young CI recipients might reach spoken word milestones with fewer months of robust hearing experience than documented for typically developing children. This outcome would indicate that children's ability to acquire language was not adversely affected by an early period of reduced hearing sensitivity and that the developmental gap between young CI users and their age-peers was being reduced.
Such relatively rapid progress would likely be facilitated by developmental advancements and experiences that supported spoken language acquisition prior to implantation. For example, toddlers who receive implants would have already undergone a restructuring of the vocal tract at approximately 4 months of age (Kent, 1984). This restructuring results in an adult-shaped vocal tract that is capable of producing recognizable vowels and consonants. Thus young CI recipients should be able to approximate adult speech models more closely than infants during the first 4 months of life. Similarly, improvements in neuro-motor control can be seen as repetitive movements of the limbs, fingers, neck and trunk reach their peak around 6 months of age in infants who are typically developing (Thelen, 1981). These coordinated behaviors are soon followed by the emergence of repetitive speech movements (i.e., canonical babbling; Kent, 1994). Young CI recipients might increase their production of repetitive speech movements soon after CI activation, in part, because they have already made gains in neuro-motor control of the speech mechanism. Infants and toddlers who are typically developing also become aware of communicative routines as they participate in interactions with family members. Young children with hearing loss participate in such exchanges as well, and these experiences are likely to increase their understanding of the intentions of social interactions. In summary, although intensive research is needed to identify the extent of their contributions, it seems reasonable to assume that pre-implant advancements in physical, cognitive, and social maturity, along with auditory experiences provided by hearing aids, and intervention efforts, would prime young CI recipients for acquiring speech and language skills once robust hearing becomes available.
A third outcome might occur if an early period of reduced hearing sensitivity or other factors have negative impacts on language acquisition. For example, children might require greater-than-typical amounts of robust hearing experience to reach spoken word milestones if substantial auditory stimulation during the first years of life is critical for language development. Slow progress might also occur if children have secondary disabilities in addition to hearing loss (Ertmer, Young, & Nathani, 2007) or if they experience frequent or prolonged CI breakdowns (Ertmer, Leonard, & Pachuillo, 2002).
A Theoretical Framework for Examining Post-implantation Language Development
Spoken language development is a complex and dynamic process in which children acquire linguistic knowledge and a variety of prelinguistic, semantic, syntactic, morphologic, and pragmatic skills over time. The Neurolinguistic theory (Locke, 1997) provides a functional and comprehensive framework for studying this process because it integrates physiological, linguistic, and developmental evidence, provides a multi-level depiction of language acquisition, proposes underlying neurological processes responsible for advancements, and specifies age ranges for the onset of key linguistic abilities. This model consists of four interdependent and overlapping phases. These phases are posited to occur in a fixed sequence, with each enabling the work of the succeeding phase. The unique ontogenetic functions of each phase are described next.
During the Vocal Learning phase (prenatal onset), infants who are typically developing “become acquainted with the vocal cues that identify people, regulate social behavior, and superficially characterize the expression of their native language” (Locke, 1997, p. 271). This task is presumed to be accomplished through innate, genetically driven mechanisms located in the right cerebral hemisphere. During the Utterance Acquisition phase (onset 5 – 7 months), infants focus on the vocal characteristics of the ambient language and store words and phrases in the right cerebral hemisphere. These stored utterances do not require and are not subjected to grammatical analysis for comprehension or production. Once “an enormous sample” (p. 273) of words and phrases and linguistically relevant data has been stored, children enter the Structure Analysis and Computation phase (onset 20 – 37 months). During this phase, the regularities of language are broken into smaller pieces by locating recurring elements across utterances and learning rules for parsing and synthesizing information. This process is presumed to be driven by mechanisms in the left cerebral hemisphere. Children enter the fourth phase, Integration and Elaboration, after 36 months of age and develop systematic grammatical rules based on the structural analysis of their stored forms and incoming language. The activities of this final phase are also attributed to left hemispheric processes that enable children to organize and integrate incoming utterances and expand lexical, morphological, phonological, and syntactic knowledge.
According to the onset ages predicted for each phase of the Neurolinguistic model, children who are implanted by 24 months would first experience robust hearing beyond the typical onset of the Vocal Learning phase. Whereas the impact of late auditory entry into this phase is not addressed by the theory, some of the genetically driven tasks of this first phase would have been undertaken prior to implantation. For example, although children who have congenital hearing losses experience limited auditory access to speech models prenatally and during the first months of life, they are likely to gain social knowledge through the sense of vision and through participating in frequent interactions with family members (e.g., feeding routines and face-to-face exchanges). Some children might also perceive low-frequency intonation and speech timing information via their hearing aids. Thus, the work of the Vocal Learning phase – becoming acquainted with the social behavior and vocal cues that are associated with language – might begin before CI fitting. If acquainted with these aspects prior to implantation, it seems reasonable to expect that young CI recipients would be prepared to enter the Utterance Acquisition phase soon after their implants are activated.
The work of the Utterance Acquisition phase is to amass the very large inventory of spoken words and phrases. This phase is believed to begin between 5 and 7 months of age. As few children are implanted at such young ages, almost all CI recipients would enter this phase after the predicted onset age. Locke estimates that the Utterance Acquisition phase continues for18 - 31 months in typically developing children. If the work of the preceding phase, Vocal Learning, has not been unduly delayed or prolonged, children who receive CIs before 24 months should begin to acquire and store utterances within the same age-range as children who are typically developing. There would be, however, an apparent advantage for implantation early in life. That is, children who receive CIs at relatively younger ages (e.g., ∼12 months) would have more time to store utterances for entry into the next phase within the predicted typical age range than children implanted later in life (e.g., ∼24 months). Entry into the Analysis and Computation phase within the typical age-range would presumably enable children to progress through the final phase of development: Integration and Elaboration (onset after 36 months). Children who enter the last three phases at near-typical ages would appear to be well-positioned to acquire age-appropriate spoken language through natural processes.
In summary, the Neurolinguistic theory provides a useful framework for examining early semantic growth within a continuum of pre-linguistic and linguistic abilities. According to this theory, children who receive CIs within the age-range for the Utterance Acquisition phase of development would be expected to show substantial increases in the number of words they understand and say. If such gains exceed typical progress during the first years of life, it would support the notion that the CI recipient's physical, cognitive, and social maturity levels, along with any pre-implant auditory experiences and intervention efforts, had primed them for spoken language development. Conversely, young CI recipients who store words and phrases at slower than typical rates might not develop an adequate vocabulary for entry into the Analysis and Computation phase within the predicted onset age-range. For such children “the optimal neuromaturational moment for the development of species-typical analytical mechanisms may have already begun to dissipate.” (Locke, 1997; p. 287). Locke postulates that children who are 4 – 6 years old before acquiring the vocabulary of a typical 2 year-old might be at risk for further language delays due to a weakening of the neural mechanisms that support expansion and integration of the components of language. Thus, the Neuorlinguistic theory provides age-related expectations that can be used to examine the adequacy of early-and later-emerging language abilities in children who typically developing and those who receive a CI at very young ages.
Research Questions and Hypotheses
The main aims of this investigation were to examine changes in the types of utterances produced and the time-courses for attaining spoken word milestones exhibited by a boy and a girl whose cochlear implants were activated at 11 and 21 months, respectively. The children's spoken utterances were analyzed from monthly recordings of mother-child interactions during the first year of implant experience. Estimates of vocabulary size were also obtained with the McArthur Communicative Development Inventory (MCDI; Fenson et al., 1993).
Two main questions were asked. First, “How do children's utterances change during the first year of CI use?” This question was addressed by determining the percentages of non-words, pre-words, single words, and word combinations observed during monthly recording sessions. Based on initial findings for Hannah (Ertmer, et al., 2003) and those documented in children who are typically developing by Robb et al. (1994), it was expected that non-meaningful utterances would decrease but continue to occur as spoken words emerged and became dominant. The second question was “How do the time-courses for reaching spoken word milestones after implant activation compare with those reported for typically developing children?” For this question, the amounts of robust hearing experience required to reach five spoken word milestones (i.e., first word, 4 words, 25 words, 1:1 word to non-word ratio, and word combinations) were calculated, and data from the MCDI were used to estimate of the size of spoken vocabulary after approximately 1 year of CI use. Based on the relatively rapid gains in vocal and spoken word development noted in prior investigations, and implantation within the age range of the Utterance Acquisition phase, it was hypothesized that spoken word milestones would be reached with fewer months of robust hearing experience than reported for children who are typically developing.
Methods
Participants
The two participants in the current study were selected from a group of seven young CI recipients who had provided video- and audio–recordings for a study of prelinguistic vocal development (Ertmer, Young, & Nathani, 2007). “Michael” and “Kathy” (not their real names) were chosen because they were implanted before their second birthdays (Michael at 10 months; Kathy at 20 months) and exhibited similar characteristics in terms of communication modality (oral), implant models, speech processing strategies, and CI-aided hearing levels. Pre-linguistic and segmental characteristics of Michael's post-implantation speech development were previously reported in Ertmer, Young, et al., (2002).
Michael
Michael's hearing impairment was first detected through newborn hearing screening 2 days following birth and confirmed through ABR testing at 1 month of age. Due to difficulties in obtaining reliable behavioral responses, unaided pure tone hearing thresholds were not obtained prior to cochlear implantation. Pre-implant ABR testing predicted severe-profound bilateral hearing loss. Michael was fitted with binaural hearing aids at 3 months of age. Limited responses to sound were observed during a 7 month hearing aid trial period, and he received a Clarion Multi-strategy CI at 10 months of age. His device was programmed with continuous interleaved sampling (CIS) approximately 1 month later (Chronological Age [CA]: 11 months). Visual reinforcement audiometry at 4.5 and 12 months post-activation yielded sound-field pure-tone averages of 25 and 28 dB HL, respectively, across 0.5, 1, 2, and 4 kHz.
Kathy
Kathy's hearing impairment was first identified at 10 months of age. Her better-ear unaided pure tone average was 96 dB HL across 0.5, 1, 2, and 4 kHz at that time. She received binaural hearing aids at 11 months. Visual reinforced audiometry yielded aided sound-field pure-tone averages of 65 dB HL across .25, .5, 1, and 2 kHz in the right ear with no responses above 2 kHz. Her left ear aided PTA was 63.3 dB HL for .25, .5, and 1 kHz, with no responses above 1 kHz. Following a 9 month hearing aid trial during which limited responses to sound were observed, she received a Clarion Multi-strategy CI at 20 months of age. Her implant was programmed with CIS and activated approximately 1 month later (CA: 21 months). Kathy exhibited pure-tone threshold averages of 29 - 39 dB HL across the 0.5 to 4 kHz frequency range during her first year of CI use.
Intervention services and pre-enrollment testing
Michael and Kathy participated in family-centered communication intervention services for 1-2 hours per week prior to receiving their CIs and throughout the first year of implant experience. Their intervention programs focused on increasing detection of environmental sounds and speech, and stimulating speech and oral language development. Both families used oral communication prior to implantation and throughout the course of this study. Neither child was reported to have spoken any words prior to implantation.
Two subtests of the Battelle Developmental Inventory (BDI; Newborg, Stock, & Wnek, 1984) were administered prior to implant activation in order to assess development in areas not directly influenced by hearing status or oral communication ability. The Adaptive Behaviors subtest was given to examine areas such as eating, dressing and toileting. The Motor Skills subtest was given to asses areas such as muscle control, body coordination, and locomotion. Michael scored at the 79th and 40th percentiles and Kathy at the 51st and 41st percentiles on these subtests, respectively. These scores indicated that both children were developing within normal limits in these areas. No physical or learning disabilities were reported on a Purdue University case history completed by the mothers.
Data Collection
Thirty-minute mother-child interaction sessions were video- and audio-recorded twice prior to implantation and on a monthly basis after CI activation. These recordings took place when Michael was between 12 and 24 months old and when Kathy was between 22 and 34 months old. Each recording session consisted of parent- or child-selected activities, such as looking at picture books, playing with dolls, or building with blocks. Parents were instructed to play with the child in their usual way. Recordings were made in the home with either a RCA VHS or a Sony 8mm Handycam (Model 200X) camcorder and Realistic Boundary microphones placed within three feet of the child. Mothers completed the Words and Gestures form of the McArthur Communicative Development Inventory (Fenson et al., 1993) on a bi-monthly basis once five spoken words were observed by parents. The last administration of the MCDI during the first year of CI use was at 11 months for Kathy and 12 months for Michael. These data were used to assess the size of the children's vocabularies after approximately 1 year of CI experience.
Data Analysis
Utterance Types
Child utterances were phonetically transcribed and then classified into five types to represent a range of pre-linguistic and linguistic utterances observed during the first two years of life in previous studies (Robb, et al., 1994; see Vihman 1996 for review). Operational definitions and examples for each utterance type can be found in Table 1. The categories included non-words (NW), pre-words (PW), single words (SW), partially correct word combinations (PCWC), and totally correct word combinations (TCWC). This five-level classification scheme extended the two-level system (i.e., words and non-words) used by Rob et al., (1994) so that the transition from non-meaningful to meaningful speech could be examined more closely.
Table 1.
Operational Definitions for Utterance Types (Adapted from Ertmer, Strong, & Sadagopan, 2003).
|
The five-level classification system was used in the following ways. Non-words were defined as utterances produced without any apparent attempt to communicate. These non-referential productions have been observed throughout the first 2 years of life in typically developing children (Stark, 1980; Oller, 1980). Pre-words were defined as unintelligible vocal attempts to communicate. These have been noted to emerge during the latter half of the first year of life in typically developing children (Stark, 1980). Utterances were classified as single words and word combinations when they were considered to be acceptable phonological approximations of adult words that appeared to have communicative intent (see criteria in Table 1). These forms typically emerge between 8 and 24 months of age (Bates, et al., 1987). Utterances were classified as word combinations when they were transcribed as having two or more meaningful components. Those in which all phonemes were judged acceptable matches for the adult target were classified as TCWCs; those in which some phonemes were judged acceptable and others unacceptable approximations of targets were classified as PCWCs. Finally, the numbers of SWs and word combinations (both PCWC and TCWC) were added together, and the numbers of NWs and PWs were added together to calculate word to non-word ratios, respectively.
Phonological criteria from the Grammatical Assessment of Elicited Language- Primary (GAEL-P, Moog & Geers, 1985) were used to determine whether utterances were acceptable as words. Children's productions were accepted as adequate phonological matches for words if they met two of three criteria: a vowel in the child's utterance matched a vowel in the adult word, a consonant in the child's utterance matched a consonant in the adult word, and the child's utterance contained the same number of syllables as the adult form (See criteria in Table 1). The GAEL-P criteria were used because it was anticipated that children with CIs would begin to use phonologically simple, but recognizable word approximations soon after implantation. For example, in a previous case study (Ertmer & Mellon, 2001), Hannah's mother reported that the child's first attempts to say words included an isolated /i/ for “eat” and /u/ for “two” when counting. The GAEL-P criteria are sensitive to such basic attempts to say words.
Time-courses for Reaching Spoken Word Milestones
The number of months of robust hearing required to reach five spoken word milestones was calculated for each participant. The milestones included: the first spoken word (10 - 13 months; Bates, et al., 1987; Snyder, Bates, & Bretherton, 1981); 4 words per 30-minutes by 11 – 12 months and 25 words per 30-minutes by 16 months (deBoysson-Bardies et al. (1992), 1:1 word to non-word ratio (13 – 21 months: Robb et al., 1994), and the production of word combinations (18 – 24 months: Bastes et al., 1987). The chronological ages at which each participant reached these milestones were used to determine how closely they matched the performance of their age peers.
Studies of typical spoken word development have used a variety of criteria to establish spoken word milestones. For example, Vihman and McCune (1994) required words to be produced several times before including them in the child's vocabulary, whereas the current study accepted words on their first occurrence. Vihman and colleagues (see Vihman, 1996 for review) also used phonological criteria that required more than two segments in the child's production to match the adult word, and at least one production that an untrained ear would recognize as a word. In contrast, the current study accepted utterances as words the first time they met criteria that were developed to be sensitive to the rudimentary speech attempts of children with hearing loss. These between-study differences require that the time-courses for reaching milestones in the current case studies be classified into broad categories until larger investigations yield more definitive measures. Thus, the three possible outcomes discussed previously will be used to describe--in general terms--the time-courses for reaching the selected milestones. These possible outcomes include (1) typical amounts of robust hearing experience, (2) less than typical amounts of robust hearing experience, and (3) greater than typical amounts of robust hearing experience.
Data Analysis
Four sources of data were analyzed to depict spoken language development during the first year of CI use. First, monthly percentages for each utterance type were calculated and presented in line charts. These charts were visually inspected for changes in the percentages of utterance types and for trends (increasing, decreasing, or stable) across time. Second, the number of months of robust hearing needed to reach spoken word milestones was compared to published reports for children who are developing typically. These comparisons were made to determine whether the participants exhibited typical or atypical time-courses for reaching milestones after the introduction of robust hearing. Third, comparisons by chronological age were made to explore developmental differences between the participants and their age-peers. Finally, the Words and Gestures form of the MCDI was completed according to standard instructions during the 11th and 12th month of CI experience for Kathy and Michael, respectively. The sizes of the participants' spoken vocabularies were compared to chronological age norms as a way to examine expressive vocabulary size toward the end of the first year of CI use.
Reliability
The second author broadly transcribed total of 3,618 utterances and categorized each utterance according to type. A senior in Speech, Language, and Hearing Sciences at Purdue University assisted with reliability measures. The student had very little prior exposure to the speech of children with hearing loss, had completed a course in phonetics, and was trained to use the utterance analysis criteria. Following this training, 3-minute segments (10% of each recorded session) were randomly chosen to assess both intra- and inter-judge reliability for each child. A total of 286 utterances were re-categorized for type during this process. Cohen's Kappa (Cohen, 1960), a statistic that corrects for chance agreement among judges, was then calculated to assess the reliability of the original classification decisions. Kappa values of 0.74 and 0.77 were obtained for intra-judge and inter-judge agreement on utterance type, respectively. Fleiss (1981) characterized Kappa values of 0.60 – 0.75 as “good” and those >0.75 as “excellent.”
Results
Utterance Types
Figure 1 displays the percentages of each utterance type produced by Michael during the first 12 post-activation months. Visual inspection of this figure shows that non-words were dominant for the first three months of CI use but decreased to very low levels after 10 months of CI use. Pre-words began to emerge as Michael attempted to convey meaning through speech during months 4 -12. His first single word was observed during month 1, but words remained infrequent until after month 5. Michael's utterances consisted mainly of pre-words and single words during the last 3 months of the study. Word combinations remained infrequent during the first year of CI use. Michael's data show an overlap between non-words, pre-words, and spoken words throughout the first year of CI use with a trend toward increasing production of recognizable words.
Figure 1.

Percentage of Utterance Types by Month for Michael. (NW: Non-words, PW: Pre-words, SW: Single Words, PCWC: Partially Correct Word Combinations, TCWC: Totally Correct Word Combinations). Filled shapes represent utterances that were identified as containing words. Michael was between 12 and 24 months old during the study.
Figure 2 shows that Kathy's first seven months of implant use were characterized by the infrequent production of non-words and the dominance of pre-words. Unlike Michael, she frequently attempted to use pre-words to communicate during the initial months of CI experience. Kathy was credited with her first word in month 1 and gradually increased single words until they accounted for nearly half of all her utterances during the last two months of the study. Word combinations emerged after four months of device use and steadily increased until they accounted for over 20% of all vocalizations in month 12. Approximately 62% of Kathy's utterances contained recognizable words (i.e., were SW, PCWC, or TCWP) one year after CI activation. The data in Figure 2 show an overlap between non-meaningful and spoken word productions, however, the paucity of non-words and steady decreases in pre-words suggest that Kathy was more advanced in communication ability at the start of the study than Michael.
Figure 2.

Percentage of Utterance Types by Month for Kathy. (NW: Non-words, PW: Pre-words, SW: Single Words, PCWC: Partially Correct Word Combinations, TCWC: Totally Correct Word Combinations). Filled shapes represent utterances that were identified as containing words. Kathy was between 22 and 34 months old during the study.
Time-course for Reaching Spoken Word Milestones
Figure 3 illustrates the number of months of robust hearing needed to reach typical word production milestones for Michael (black columns) and Kathy (white columns). This figure also shows the chronological ages of the children when they reached each milestone: Michael's CA is represented by dark gray columns; Kathy's by light gray columns. The dotted lines show the range of typical attainment or the mean age of attainment for each milestone. The black and white columns in Figure 3 show that both children reached each of the five milestones with fewer months of robust hearing experience than documented for children who are typically developing. The first- and four-word milestones were accomplished with the fewest months of robust hearing (1 month post-CI activation); the attainment of a 1:1 non-word to word ratio required the most months of robust hearing (12 for Michael; 11 for Kathy). In general, the two participants took similar amounts of time after implant activation to reach most milestones although Kathy began to produce two-word combinations with 5 fewer months of robust hearing experience than Michael.
Figure 3.
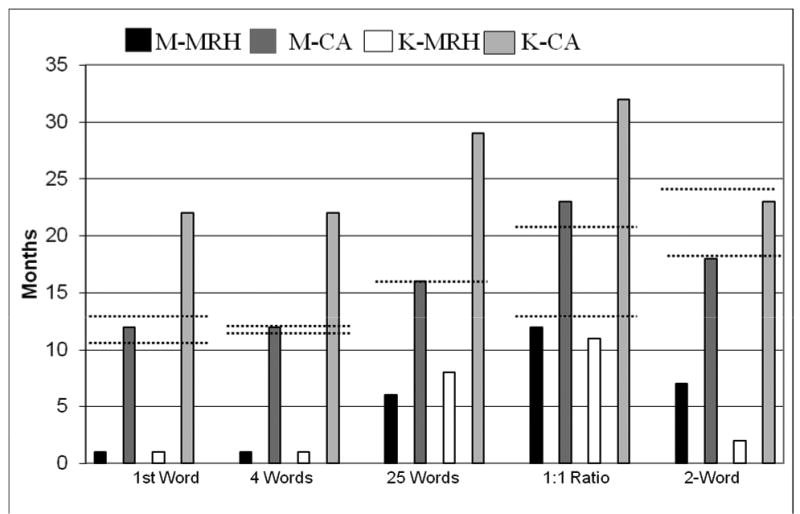
Comparisons of the Time-courses for Reaching Spoken Word Milestones according to Months of Robust Hearing (MRH) Experience and Chronological Age (CA). (Black columns and dark gray columns represent MRH and CA, respectively, for Michael. White columns and light gray columns represent MRH and CA, respectively, for Kathy.)
Figure 3 also shows comparisons between the typical chronological ages of attainment for each milestone and the participant's actual chronological age (CA) when milestones were reached. Michael's CA (dark gray columns) was very close to the typical age range when he reached the first word, 4 words, 25 words, and two-word combination milestones. He was slightly older (23 months) than the age range of the children studied by Robb et al., (1994) when he reached the 1:1 word to non-word ratio. In contrast, Kathy achieved only the two-word combination milestone within a typical age range (see light gray columns). The remaining milestones were achieved an average of 10.8 months after the typical age of attainment.
Robb et al., (1994) found that children who are typically developing showed a large increase in word production and reached a 2:1 ratio of single words to non-words within a month after reaching the 1:1 ratio (i.e., 13 - 21 months of age). In the current study, Michael reached the 1:1 ratio at 12 months. It was not determined, however, when he experienced a sizable increase in spoken words vs non-words because data analysis was discontinued at that point. Kathy produced 111 single words to 90 non-words after 11 months of robust hearing experience (CA = 32 months), achieving the 1:1 ratio in fewer robust hearing months than the toddlers in the Robb et al. (1994) study. Data from the following month showed only a slight increase to a ratio of 1.18:1, indicating that Kathy did not reach the 2:1 ratio as quickly as the children in the Robb study.
Maternal reports using the MCDI (Fenson et al., 1993) indicated that each child had acquired a substantial spoken vocabulary. Michael was reported to say and understand 241 words after 12 months of robust hearing. This amount of words was equated 50 - 55th percentile for boys of the same chronological age (23 months). Kathy was reported to say and understand 346 words after 11 months of robust hearing. Her CA at this point (33 months) exceeded the upper age limits of the MCDI norms for toddlers (i.e., 30 months) however, her spoken vocabulary of 346 words was approximated the 20th percentile for girls at 30 months (Fenson et al., 1993). Thus, after approximately 1 year of CI use, the size of Michael's spoken vocabulary was within normal limits for his age and it was inferred that Kathy's was smaller than expected for children of her age. Thus, Michael's younger age at implantation appeared to negate any spoken vocabulary gap with peers. Although Kathy acquired more words than Michael during the first year of robust hearing, she continued to be behind her peers in vocabulary development.
According to Bates, O'Connell, & Shore (1987), TD children begin to produce two-word combinations between 18 - 24 months of age. Michael and Kathy were observed to produce two word combinations by 7 and 2 months after CI activation, respectively. Thus, they required much less robust hearing experience than typically needed to reach this milestone. Each child began to produce word combinations within the typical chronological age-range (Figure 3).
Taken together, the relatively rapid attainment of most spoken word milestones and the large vocabularies noted on the MCDI, support the hypotheses that (a) the children were primed for language acquisition by pre-implantation maturational processes and hearing experiences, and (b) the introduction of robust hearing within the proposed age-range for the Utterance Acquisition phase of Neurolinguistic theory (Locke, 1997) was beneficial for storing a substantial vocabulary of spoken words.
Discussion
How did the children's utterances change during the first year of CI use?
A major finding of this investigation was that both children became more consistent oral communicators during the first year of robust hearing. Non-communicative and unintelligible utterances (non-words) accounted for approximately 90% of Michael's utterances during the first 3 months of CI experience. It was not long, however, before increases in communicative attempts were noted: pre-words increased sharply to 50% in month 4 and remained at comparable levels throughout the remainder of the study. The sudden increase and stability of pre-words indicated that Michael used vocalizations to convey his ideas more frequently, even if they could not be readily understood. Michael's first single words were observed during month 1 (CA = 12 months) and single words increased gradually until they accounted for 40 – 45% of his utterances during months 9 – 12. More than 95% of his utterances were communicative (i.e., pre-words, single words, and word combinations) during the last three months (Figure 1).
For Kathy, non-words were relatively infrequent (3 – 16%) across the first year of CI use. It was interesting to note, however, that non-words continued to be produced and actually increased during the last 4 months of the study. The continued production of these forms suggests that self-directed vocal experimentation might have continued even after single words became common—an observation that also applies to Michael during months 6 – 9. Kathy, however, appeared to have been more advanced than Michael in her use of spoken communication attempts at the start of the study. This can be seen as pre-words dominated the first 8 months of CI use (ranging from 57-87%). Her high percentage of pre-words during the first month of CI use suggests that she might have produced pre-words prior to implantation. This possibility was confirmed through a post hoc analysis that revealed that 6 of 280 utterances were pre-words (∼2%) prior to CI activation. The remaining vocalizations were non-words. In contrast, all of Michael's pre-implantation utterances were classified as non-words. Thus, Kathy's more advanced communicative ability may have been related to her relatively older age when implanted. Kathy, like Michael, produced single words during the first post-activation recording session (CA = 22 months). Her single words and word combinations increased gradually; eventually accounting for approximately half of her utterances during months 11 and 12. As Figure 2 shows, spoken words had become Kathy's most common utterance type after one year of robust hearing experience.
In answer to our first research question, the first year of robust hearing was characterized by the emergence and increasing production of meaningful utterances and a decreasing but continued production of non-meaningful speech. Whereas this description is similar to the progression seen in typically developing youngsters using a word vs non-word dichotomy (Robb et al, 1994), the five-level classification system used in the current study (i.e., NW, PW, SW, PCWC, and TCWC) permitted a closer look at this transition in two new ways.
First, by considering children's communicative intent, the system was able to track changes in the percentages of non-communicative vocalizations and those produced with apparent communicative intent. Michael made substantial strides in this area as pre-words and single words increased after the third month of CI use. In this way, the distinction between non-words and pre-words revealed an important change in the functions of Michael's utterances. For Kathy, the five-level system permitted tracking of the emergence of single words and word combinations to a greater extent than the transition from non-word to pre-word dominance.
The five-level classification system also permitted tracking of improvements in intelligibility. This can be seen most clearly in the decline of pre-words and the concurrent increase in single words for most of Kathy's sessions, and, to a lesser degree, in similar trends observed during months10 – 12 for Michael. These trends are compatible with the Robb et al., (1994) conclusion that single word stage reflects the onset of more intelligible utterances. Thus, as seen in children who are typically developing, phonological advancements appeared to pave the way for the emergence of words. Further study is needed to determine whether similar trends are observed in other young CI recipients.
Clinical Implications
The five-level classification system can also be useful in clinical practice. Specifically, parent-child interactions can be analyzed to assess progress in communicative and spoken word development by tracking the percentages of non-words, pre-words, single words, and word combinations during the first year of CI use. Advancements in communicative and early linguistic abilities can be documented as children decrease non-word production, increase and then decrease pre-words, and produce increasingly greater proportions of recognizable words. Combining this information with parent report instruments such as the MCDI (Fenson et al., 1993) and parent diaries (Nott et al., 2006) can help to verify CI benefit for children who are too young to participate in structured assessments. In addition, by alerting parents to pre-words and phonologically simplified single words, families can learn to reinforce and stimulate the development of meaningful speech during the initial months of CI use.
“How do the time-courses for reaching spoken word milestones after implant activation compare with those reported for children who are typically developing?
Comparisons with children who are typically developing were made to determine whether post-implantation development could be characterized as requiring typical amounts of robust hearing experience, fewer months than typical, or more months than typical. These comparisons should be interpreted cautiously because studies of typically developing children have used differing contextual and phonological criteria to identify words. In light of these differences, the following comparisons must be considered preliminary estimates of the time-course for the transition from mainly pre-linguistic utterances to spoken words after cochlear implant activation.
Comparisons by Amount of Robust Hearing
Michael and Kathy reached five spoken word milestones with less than typical amounts of robust hearing experience (Figure 3). In the cases of the first word, 4 words per 30 minute samples, 25 words in 30 minute samples, and 2-word combination milestones, Michael required between 9 and 11 fewer months of robust hearing than typically developing children; Kathy required between 8 and 16 fewer months. In answer to the second research question, the participants clearly required fewer months of robust hearing to reach these milestones than is reported for children who are typically developing.
In contrast, both required near typical amounts of robust hearing experience to reach the 1:1 word : non-word ratio. Michael reached this milestone within one month, and Kathy within 2 months of the expected range for typically developing children (13 – 21 months). This finding suggests that while the first spoken words emerged relatively rapidly, achieving a balance between words and non-words required extended amounts of robust hearing experience. Additionally, Kathy did not reach the 2:1 ratio during the month after reaching the 1:1 level (as seen in the Robb study) and, therefore, did not achieve this shift toward spoken word dominance as rapidly as typically observed. Recall that this milestone was not examined for Michael because data analysis ended at one year post-activation. Further study of the 2:1 word to non-word ratio is needed to explore the transition from a balance between non-words and words to spoken word dominance.
Maternal reports indicated that Michael and Kathy said 244 and 346 different words, respectively, near the end of the study. Data from the Words and Gestures form of the MCDI indicate that, on average, boys produce 3 words and girls produce 4 words at 12 months of age (50th percentile; Fenson et al., 1993). Thus, the participants acquired a much larger spoken vocabulary during the first year of robust hearing experience than is typical for infants during the first year of life. The participants' relatively rapid advancements are similar to those noted in studies of prelinguistic vocal development (e.g., Ertmer et al., 2007; Mcaffrey et al., 1999; Moore & Bass-Ringdahl, 2002), and vocabulary during the first year of CI use (Ertmer & Mellon, 2001). As Vihman (1996) noted, “Certain anatomical and neuro-motor factors undoubtedly play a critical role in pacing the development of vocal behavior.” (p. 118). The participants' rapid progress in these areas suggests that their relatively advanced physical, cognitive, and social maturity, along with pre-implant hearing experiences, primed them for integrating auditory information, a speech movement system, and spoken language.
Theoretical considerations
The current findings are compatible with the Neurolinguistic theory (Locke, 1997). Both children received robust hearing within the predicted age range for the Utterance Acquisition phase (estimated duration: 5 – 37 months). Whereas it cannot be known for certain, their rapid gains in word production appear to indicate that they had become acquainted with the vocal cues associated with people and social interactions during the preceding phase of development: Vocal Learning. Advances during this earliest phase of development may have been accomplished through a variety of mechanisms including visual learning, social experiences, pre-implant experiences with hearing aids, robust hearing via a CI, or a combination of these factors.
Direct observation and parent report confirm that both participants had made substantial progress toward acquiring the enormous sample of words or phrases that is the unique ontogenetic function of the Utterance Acquisition phase (Locke, 1997). Michael, because he was younger than Kathy when implanted, had more time to acquire and store utterances for entry into the next phase (Analysis and Computation) within the predicted age-range. Kathy, although implanted at a comparatively older age, acquired a larger vocabulary than Michael during the first year of CI use. Thus, she appeared to be storing words and phrases at a faster rate. Rapid increases in spoken vocabulary size suggest that the introduction of robust hearing enabled both children to join in the work of the Utterance Acquisition phase, and so a clear advantage for a younger age at implantation was not seen in the rate at which spoken vocabulary increased. Entry into the next phase of development (Integration and Expansion) within the predicted age-range would be expected if they continue to store words and phrases expeditiously.
Support for the Neurolinguistic theory can also be found in earlier studies of children who were implanted within the proposed age range for the Utterance Acquisition phase. Hannah, the child studied by Ertmer et al., (2003), was reported to have large receptive and expressive vocabularies after one year of CI use (240 and 90 words, respectively). Connor and colleagues noted that implantation before 30 months yielded a burst of vocabulary growth that was not be matched by children implanted at older ages (Connor et al., 2006). These and the current findings are encouraging because they suggest that implantation at very young ages permits children to take advantage of natural processes that lead to age-appropriate language ability. However, language development is likely to be influenced by factors in addition to age at implantation. For example, intelligence and communication modality (Geers, 2002), amount of residual hearing prior to implantation (Szagun, 2001), and the effects of intervention might also play key roles.
Language development is a multifaceted and prolonged process in which children may exhibit variable rates of progress. Szagun (2001) found differing rates of grammatical development (measured in Mean Length of Utterance) in German-speaking children who received CIs at a mean age of 29 months. Those who made fast progress at an early stage continued to make fast progress as time went on; those who made slow progress at first continued to progress more slowly. Ertmer, et al., (2003) noted differing rates of development across later-emerging language skills within the same child. Four areas were found to be developing at normal or near normal rates (i.e., comprehension of phrases, receptive vocabulary, type-token ratio, word combinations, and decreased production of non-words), and three areas were characterized as having a below normal rate of development (speech intelligibility, number of word types and tokens produced, and mean length of utterance). Additionally, Spencer, Barker, and Tomblin (2003) reported relatively greater difficulty in formulating sentences than other language skills in school-age CI users. Taken together, these studies highlight a need to explore the rates at which early- and later-emerging linguistic abilities develop as well as interactions between these abilities in young CI recipients.
Chronological Age Comparisons
Michael's chronological age was very close to or within the typical age-range when he reached each of the five milestones examined, suggesting that he was on a typical trajectory for early spoken word development. Kathy was within the typical age-range for the emergence of word combinations only. On average, she was 10 months beyond the typical age when reaching the remaining milestones. Examination of Figure 3 reveals that Kathy and Michael reached most milestones with comparable months of robust hearing experience. The similarity of the latter time-courses suggests that Kathy achieved fewer milestones within the typical age-range because she was implanted when she was 10 months older than Michael. This finding supports the notion that children who are implanted close to their first birthdays may be able to close the gap with age peers sooner than those implanted closer to their second birthdays.
Cautions and Future Directions
Although the rapid spoken word gains of the current study suggest that language acquisition might become more normalized with continued CI use, at least two caveats should be kept in mind when predicting further progress. First, continued enrollment in special intervention programs will likely be needed to achieve and maintain age-appropriate oral communication abilities. Second, children who use CIs continue to have poorer than normal hearing sensitivity when using their devices. Research has shown that even children with minimal and mild hearing losses often experience delays in academics (Bess, Dodd-Murphy, & Parker, 1998) possibly due to ongoing language difficulties. Thus, although young CI recipients have much improved hearing sensitivity, they may experience greater difficulties in acquiring spoken language and academic skills than age peers who have normal hearing.
The findings of the current study must be viewed as preliminary until more young CI recipients can be examined. In particular, further study is needed to arrive at reliable estimates of the time-course of post-implantation spoken word development and to make methodologically equivalent comparisons between young CI recipients and children who are typically developing. Comparisons of children implanted as infants and those implanted at older ages (e.g. > 2-3 years) are also needed to help identify any advantages associated with younger ages at implantation. These larger-scale investigations must account for age-at-implantation, unaided and CI-aided hearing levels, family characteristics, and communication modality so that the contribution of these factors can be identified. Such studies will help to establish expectations for semantic, syntactic, phonological, and morphological development in very young CI recipients, assist in testing theories of spoken language development, and provide treatment insights for clinicians and families.
Conclusions
Kathy and Michael made noteworthy progress toward becoming oral communicators during their first year of robust hearing. In particular, their expeditious gains in spoken word development suggest that they were primed to integrate auditory information, speech movements, and semantics. Their readiness was apparently facilitated by their physical, cognitive, and social maturity at the time robust hearing was introduced, pre-CI hearing experiences, participation in communication intervention, and interactions among these factors. Sizable gains in spoken word development suggest that the introduction of robust hearing during the Utterance Acquisition phase enabled the children to take advantage of neurolinguistic processes that typically promote language development (Locke, 1997). Further study is needed to understand the factors that influence this complex yet elegant process in children who receive CIs at very young ages.
Acknowledgments
This research project was supported through grants from the National Institute on Deafness and other Communication Disorders (1R030DC04226-03 and R01DC007863). We are especially grateful to the children and families who participated in the study. A special thank you is extended to Leeann Schwartz for her help with reliability measures. The insightful suggestions of Karen Kirk, Mary Pat Moeller, Robert Novak, and David Snow on earlier versions of this manuscript are gratefully acknowledged.
Footnotes
Publisher's Disclaimer: This is an author-produced manuscript that has been peer reviewed and accepted for publication in the Journal of Speech, Language, and Hearing Research (JSLHR). As the “Papers in Press” version of the manuscript, it has not yet undergone copyediting, proofreading, or other quality controls associated with final published articles. As the publisher and copyright holder, the American Speech-Language-Hearing Association (ASHA) disclaims any liability resulting from use of inaccurate or misleading data or information contained herein. Further, the authors have disclosed that permission has been obtained for use of any copyrighted material and that, if applicable, conflicts of interest have been noted in the manuscript.
References
- American Speech-Language-Hearing Association. Executive summary: Cochlear implants. Technical report. ASHA Supplement. 2004;24:103–108. [Google Scholar]
- Bates E, O'Connell B, Shore C. Language and communication in infancy. In: Osofsky J, editor. Handbook of Infant Development. New York: John Wiley & Sons; 1987. pp. 149–203. [Google Scholar]
- Bess FH, Dodd-Murphy J, Parker RA. Children with Minimal Sensorineural Hearing Loss: Prevalence, Educational Performance, and Functional Status. Ear and Hearing. 1998;18:339–354. doi: 10.1097/00003446-199810000-00001. [DOI] [PubMed] [Google Scholar]
- Bollard PM, Chute PM, Popp A, Parisier SC. Specific language growth in young children using the Clarion cochlear implant. Annals of Otology, Rhinology, & Laryngology. 1999;108(4) 177:119–123. doi: 10.1177/00034894991080s424. part 2. [DOI] [PubMed] [Google Scholar]
- Carney AE, Moeller MP. Treatment efficacy: Hearing loss in children. Journal of Speech, Language, and Hearing Research. 1998;41:S61–S84. doi: 10.1044/jslhr.4101.s61. [DOI] [PubMed] [Google Scholar]
- Chin SB, Tsai PL, Gao S. Connected speech intelligibility of children with cochlear implants and children with normal hearing. American Journal of Speech-Language Pathology. 2003;12:440–451. doi: 10.1044/1058-0360(2003/090). [DOI] [PubMed] [Google Scholar]
- Cohen J. A coefficient of agreement for nominal scales. Educational and Psychological Measurement. 1960;20:37–46. [Google Scholar]
- Connor CM, Craig HK, Raudenbush SW, Heavner K, Zwolan TA. The age at which young deaf children receive cochlear implants and their vocabulary and speech-production growth: Is there added value for early implantation? Ear and Hearing. 2006;27:628–644. doi: 10.1097/01.aud.0000240640.59205.42. [DOI] [PubMed] [Google Scholar]
- Connor CM, Hieber S, Arts HA, Zwolan TA. Speech, vocabulary, and the education of children using cochlear implants: Oral or total communication. Journal of Speech, Language, and Hearing Research. 2000;43:1185–1204. doi: 10.1044/jslhr.4305.1185. [DOI] [PubMed] [Google Scholar]
- deBoysson-Bardies B, de Vihman MM, Roug-Hellichius L, Durand C, Landberg I, Arao F. Material evidence of infant selection from the target language: A cross-linguistic phonetic study. In: Ferguson CA, Menn L, Stoel-Gammon C, editors. Phonological development: Models, research, implications. Timonium, Maryland: York Press; 1992. pp. 369–391. [Google Scholar]
- Ertmer DJ. The Source for Children with Cochlear Implant. East Moline, IL: LinguiSystems, Inc.; 2005. [Google Scholar]
- Ertmer DJ, Leonard JS, Pachuillo MP. Communication intervention for children with cochlear implants: Two case studies. Language Speech and Hearing Services in the Schools. 2002;33:205–217. doi: 10.1044/0161-1461(2002/018). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Mellon JA. Beginning to talk at 20 months: Early vocal development in a young cochlear implant recipient. Journal of Speech, Language, and Hearing Research. 2001;44:192–206. doi: 10.1044/1092-4388(2001/017). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Strong LM, Sadogopan N. Beginning to communicate after cochlear implantation: Oral language development in a young child. Journal of Speech, Language, and Hearing Research. 2003;46:328–340. doi: 10.1044/1092-4388(2003/026). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Young NM, Grohne K, Mellon J, Johnson C, Corbett K, Saindon K. Vocal development in young children with cochlear implants: Profiles and implications for intervention. Language, Speech and Hearing Services in the Schools. 2002;33:184–195. doi: 10.1044/0161-1461(2002/016). [DOI] [PubMed] [Google Scholar]
- Ertmer DJ, Young NM, Nathani S. Vocal development in young children with cochlear implants: A preliminary examination of sequence, time-course, and age-at-implantation. Journal of Speech, Language, and Hearing Research. 2007;50:393–407. doi: 10.1044/1092-4388(2007/028). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fenson L, Dale P, Resnick J, Bates E. MacArthur Communication Development Inventories: User's Guide and Manual. San Diego: Singular; 1993. [Google Scholar]
- Fleiss JL. Statistical methods for rates and proportions. New York: Wiles; 1981. [Google Scholar]
- Fletcher P. Speech and Hearing in Communication. Princeton: D. VanNostrand Co.; 1953. [Google Scholar]
- Fletcher P, Garman . Introduction to Part 1. In: Fletcher P, Garman M, editors. Language acquisition: Studies in first language development. Cambridge: Cambridge University Press; 1979. [Google Scholar]
- Fryauf-Bertschy H, Tyler RS, Kelsay PMR, Gantz BJ, Woodworth GG. Cochlear implant use by prelingually deafened children: The influences of age at implant and length of use. Journal of Speech, Language, and Hearing Research. 1997;40:183–199. doi: 10.1044/jslhr.4001.183. [DOI] [PubMed] [Google Scholar]
- Geers AE. Factors affecting the development of speech, language, and literacy in children with early cochlear implantation. Language, Speech, and Hearing in the Schools. 2002;33:172–183. doi: 10.1044/0161-1461(2002/015). [DOI] [PubMed] [Google Scholar]
- Geers A, Brenner C, Davidson L. Factors associated with development of speech perception skills in children implanted by age five. Ear and Hearing. 2003;24:24S–35S. doi: 10.1097/01.AUD.0000051687.99218.0F. [DOI] [PubMed] [Google Scholar]
- Ingram D. First Language Acquisition: Method, Description, and Explanation. New York: Cambridge University Press; 1989. [Google Scholar]
- Kent RD. Psychobiology of speech development: Co-emergence of language and a movement system. American Journal of Physiology. 1984;246:R888–R894. doi: 10.1152/ajpregu.1984.246.6.R888. [DOI] [PubMed] [Google Scholar]
- Kent RD. The biology of phonological development. In: Ferguson C, Menn L, Stoel-Gammon C, editors. Phonological Development: Models, Research, and Implications. Timonium, MD: York Press; 1994. [Google Scholar]
- Locke J. A theory of neurolinguistic development. Brain and Language. 1997;58:265–326. doi: 10.1006/brln.1997.1791. [DOI] [PubMed] [Google Scholar]
- McCaffrey HA, Davis BL, MacNeilage PF, von Hapsburg D. Multichannel cochlear implantation and the organization of early speech. Volta Review. 1999;101:5–28. [Google Scholar]
- Miyamoto RT, Kirk KI, Svirsky MA, Sehgal ST. Communication skills in pediatric cochlear implant recipients. Acta Oto-Laryngologica. 1999;119(2):219–224. doi: 10.1080/00016489950181701. [DOI] [PubMed] [Google Scholar]
- Moog JS, Geers AE. Grammatical analysis of elicited language. St. Louis, MO: Central Institute for the Deaf; 1985. [Google Scholar]
- Moore JA, Bass-Ringdahl S. Infant vocal development in candidacy for and efficacy of cochlear implantation. Annals of Otology, Rhynology, and Laryngology. 2002;111:52–55. doi: 10.1177/00034894021110s511. [DOI] [PubMed] [Google Scholar]
- Nathani S, Ertmer DJ, Stark RE. Assessing vocal development in infants and toddlers. Clinical Linguistics and Phonetics. 2006;20:351–369. doi: 10.1080/02699200500211451. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newborg J, Stock JR, Wnek L. Battelle Developmental Inventory. 1st. Itaska, IL: Riverside Publishing; 1984. [Google Scholar]
- Nicholas JG, Geers AE. Hearing status, language modality, and young children's communicative and linguistic behavior. Journal of Deaf Studies and Deaf Education. 2003;8:422–437. doi: 10.1093/deafed/eng029. [DOI] [PubMed] [Google Scholar]
- Nikolopolous TP, O'Donoghue GM, Archbold SM. Age of implantation: Its importance in pediatric cochlear implantation. Laryngoscope. 1999;109(4):595–599. doi: 10.1097/00005537-199904000-00014. [DOI] [PubMed] [Google Scholar]
- Oller DK. The emergence of the sounds of speech in infancy. In: Yeni-Komshian G, Kavanaugh J, Ferguson C, editors. Child Phonology. Vol. 1. New York: Academic Press; 1980. pp. 93–112. [Google Scholar]
- Oller DK, Eilers R. The role of audition in infant babbling. Child Development. 1988;59:441–449. [PubMed] [Google Scholar]
- Robb MP, Bauer HR, Tyler AA. A quantitative analysis of the single-word stage. First Language. 1994;14:37–48. [Google Scholar]
- Schauwers K, Gillis B, Daemers K, de Beukelaer C, Govaerts PJ. Cochlear implantation between 5 and 20 months of age: The onset of babbling and the audiologic outcome. Otology and Neurotology. 2004;25:263–270. doi: 10.1097/00129492-200405000-00011. [DOI] [PubMed] [Google Scholar]
- Snyder L, Bates E, Bretherton I. Content and context in early lexical development. Journal of Child Language. 1981;8:565–582. doi: 10.1017/s0305000900003433. [DOI] [PubMed] [Google Scholar]
- Spencer PE. Individual differences in language performance after cochlear implantation at one to three years of age: Child, family, and linguistic factors. Journal of Deaf Studies and Deaf Education. 2004;9:395–412. doi: 10.1093/deafed/enh033. [DOI] [PubMed] [Google Scholar]
- Spencer LJ, Barker BA, Tomblin JB. Exploring the language and literacy outcomes of pediatric cochlear implant users. Ear & Hearing. 2003;24:236–247. doi: 10.1097/01.AUD.0000069231.72244.94. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stark RE. Stages of speech development in the first year of life. In: Yeni-Komshian G, Kavanaugh J, Ferguson C, editors. Child Phonology. Vol. 1. New York: Academic Press; 1980. pp. 73–90. [Google Scholar]
- Szagun G. Language acquisition in young German-speaking children with cochlear implants: Individual differences and implications for conceptions of a “sensitive period”. Audiology & Neuro-Otology. 2001;6:288–297. doi: 10.1159/000046134. [DOI] [PubMed] [Google Scholar]
- Tait M, Lutman ME, Robinson K. Preimplant measures of preverbal behaviors as predictors of cochlear implant outcomes in children. Ear & Hearing. 2000;21:18–24. doi: 10.1097/00003446-200002000-00005. [DOI] [PubMed] [Google Scholar]
- Thelen E. Rhythmical behavior in infancy: An ethological perspective. Developmental Psychology. 1981;17:237–257. [Google Scholar]
- Tomblin JB, Barker BA, Spencer LJ, Zhang X, Gantz BJ. The effect of age at cochlear implant initial stimulation on expressive language growth in infants and toddlers. Journal of Speech, Language, and Hearing Research. 2005;48:853–867. doi: 10.1044/1092-4388(2005/059). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Vihman MM. Phonological Development: The Origins of Language in the Child. Cambridge, MA: Blackwell Publishers; 1996. [Google Scholar]
- Vihman M, Mc Cune L. When is a word a word? Journal of Child Language. 1994;21:517–542. doi: 10.1017/s0305000900009442. [DOI] [PubMed] [Google Scholar]
- Vihman MM, Miller R. Words and babble at the threshold of language acquisition. In: Smith MD, Locke JL, editors. The Emergent Lexicon: The Child's Development of a Linguistic Vocabulary. New York: Academic Press; 1988. pp. 151–183. [Google Scholar]