

Abstract
In this paper, preterm infant massage therapy studies are reviewed. Massage therapy has led to weight gain in preterm infants when moderate pressure massage was provided. In studies on passive movement of the limbs, preterm infants also gained significantly more weight, and their bone density also increased. Research on ways of delivering the massage is also explored including using mothers versus therapists and the added effects of using oils. The use of mothers as therapists was effective in at least one study. The use of oils including coconut oil and safflower oil enhanced the average weight gain, and the transcutaneous absorption of oil also increased triglycerides. In addition, the use of synthetic oil increased vagal activity, which may indirectly contribute to weight gain. The weight gain was associated with shorter hospital stays and, thereby, significant hospital cost savings. Despite these benefits, preterm infant massage is only practiced in 38% of neonatal intensive care units. This may relate to the underlying mechanisms not being well understood. The increases noted in vagal activity, gastric motility, insulin and IGF-1 levels following moderate pressure massage are potential underlying mechanisms. However, those variables combined do not explain all of the variance in weight gain, highlighting the need for additional mechanism studies.
Approximately 14% of infants in the United States are born prematurely (National Center for Health Statistics, 2007). Prematurity, in turn, is one of the leading causes of infant morbidity and mortality, and it results in approximately 15.5 billion dollars in hospital costs per year. Following intensive care treatment, weight gain becomes the main criterion for hospital discharge. Thus, several interventions have been designed to promote preterm infant weight gain including massage therapy.
Massage Therapy Studies
Randomized, controlled studies have documented greater weight gain in preterm newborns receiving moderate pressure massage therapy (see Field, Hernandez-Reif & Freedman, 2004; Vickers, Ohlsson, Lacy & Horsley, 2004 for reviews). These include our studies on preterm newborns who received 5-10 days of massage therapy and showed a 21-48% greater increase in weight gain and hospital stays of 3-6 days less than control infants (Diego, Field & Hernandez-Reif, 2005; Dieter, Field, Hernandez-Reif, Emory & Redzepi, 2003; Field, Schanberg, Scafidi, Bauer & Vega-lahr, 1986; Scafidi, Field, Schanberg, Bauer & Vega-Lahr, 1990; Wheeden, Scafidi, Field, Ironson & Valdeon, 1993) (see table 1). These weight gain findings have been replicated by at least 4 independent groups (Cifra & Sancho, 2004; De-Roiste & Bushnell, 1996; Goldstein-Ferber, Kuint, Weller, Feldman, Dollberg, Arbel & Kohelet, 2002; Mathai, Fernandez, Modkar & Kanbur, 2001).
Table 1.
Mean weight gain for our massage therapy studies (s.d.s in parentheses).
| Weight Gain/Day (g) | |||||
|---|---|---|---|---|---|
| #Days | Massage | Control | p | %Wt Gain | |
|
Field et al., 1986 (n = 40) |
10 | 25.0 (6.0) |
17.0 (6.7) |
.005 | 47 |
|
Scafidi et al., 1990 (n = 40) |
10 | 33.6 (5.4) |
28.4 (11.1) |
.003 | 21 |
|
Wheeden et al., 1993 (n = 30) |
10 | 33.0 (7.3) |
25.7 (7.0) |
.009 | 27 |
|
Dieter et al., 2003 (n = 32) |
5 | 48.7 (36.9) |
32.7 (12.2) |
.01 | 48 |
|
Diego et al., 2005 (n = 32) |
5 | 19.6 (3.9) |
15.5 (3.7) |
.01 | 25 |
The 2 groups in each study were equal Ns S.Ds are in parentheses.
The protocol in our randomized, controlled studies on the effects of massage therapy on NICU preterm infants involves moderate pressure stroking (tactile stimulation) and flexion and extension of the upper and lower extremities (kinesthetic stimulation) (see Field, Hernandez-Reif & Freedman, 2004 for a review). These sessions have varied between 10 and 15 minutes and have been held two to three times a day for 5-to-10-days. All studies have reported greater weight gain for the massage therapy versus the standard care control group.
In our early studies (Field et al. 1986; Scafidi et al., 1990; Wheeden et al., 1993) a 15-minute massage therapy protocol, three times per day, for ten days resulted in 21-47% greater weight gain than standard care alone (see Table 1). Those infants were also discharged six days earlier on average than control infants, saving approximately ten thousand dollars in hospital costs per infant. Examination of the daily weight gain curves across the 10-day treatment period revealed that the massaged infants exhibited greater weight gain than the control infants as early as day 5 in the 10-day study, suggesting that 5 days of massage might be sufficient to increase weight gain at a reduced cost. In a study assessing the shorter time period, preterm infants receiving only 5 days of massage therapy gained 48% more weight than control infants (Dieter et al., 2003; Table 1).
In a recent study by a research group in India, the same protocol resulted in a weight gain of 4.24 grams per day more than controls (Mathai, et al, 2001). On the Brazelton Scale the massage group showed statistically higher scores on the orientation, range of state, regulation of state and autonomic stability subscales. In a meta-analysis of several studies using the same protocol, massage increased the daily weight gain by 5.1 grams on average (Vickers et al, 2004), reduced the length of hospital stay by 4.5 days and had a positive effect on postnatal complications as well as weight gain at 4-6 months.
Other replications using this infant massage protocol were conducted in China. These studies also documented significant weight gain (Duan, Li & Shi, 2002; Ke, Ling & Li, 2001; Liu, 2005; Liu Chun Li, 2005; Lu Jiao, Li Ju Zhan & Wu Li Fang, 2005; Na Zhuo Hua, Zie Hui Yun & Huang Jian Hua, 2005; Shi Li & Xue Li Rong, 2002; Sun Hai Yun, Gao Xiang Yu & Zhao Xue Mei, 2005; Zhai, J., Pan Xian, R. & Hua, J.R., 2001). Some of these studies also reported increased length and head circumference (Duan et al, 2002; Ke, Ling, 2001; Liu, 2005; Lu Jiao et al, 2005; Na et al, 2005).
Exercise Studies
Greater weight gain has also been observed in preterm infants receiving passive limb movements. This exercise, which is a form of stimulation similar to the kinesthetic component of our massage protocol, involves flexing and extending the limbs (Eliakim, Nemet, Friedland, Dolfin & Regev, 2002; Moyer-Mileur, Brunstetter, McNaught, Gill & Chan, 2000; Nemet, Dolfin, Litmanowitz, Shainkin-Kestenbaum, Lis & Eliakim, 2002). The weight gain in these studies was less than in the massage therapy studies (0-38%). However, the exercise sessions in these studies were shorter than the typical 15 minute massage sessions, and they were held only once per day. Nonetheless, the infants showed increased bone mineral density. Thus, exercise or the kinesthetic form of stimulation appears to lead to weight gain (see table 2) as well as bone growth in preterm infants (Eliakim et al, 2002; Moyer-Mileur, Luetkemeier, Boomer & Chan, 1995, 2000; Nemet et al, 2002).
Table 2.
Effects of Preterm Infant Exercise on Weight Gain (S.D.s. in parentheses) Weight Gain/Day (g)
| Exercise | Control | p | % Weight Gain | |
|---|---|---|---|---|
| Moyer-Mileur et al. (1995) | 17.8 (2.8) |
13.4 (2.8) |
.001 | 38 |
| Moyer-Mileur et al. (2000) | 16.3 (2.6) |
14.6 (2.0) |
.02 | 20 |
| Nemet et al. (2002) | --- | --- | .05 | 31 |
Preterm infants are at risk for developing bone disease and bone fractures due to the limited formation of bone mass in utero and to limited activity (Backstrom, Kuusela & Maki, 1996; Rigo, De Curtis, Pieltain, Picaud, Salle & Senterre, 2000). Inactivity has been associated with decreased bone mineral density (Rodriguez, Garcia, Palacios & Paniagua, 1988), and physical activity promotes bone development (Myburgh, 1998). The passive movement or exercise of preterm infants' limbs has increased serum bone formation markers, most especially bone specific alkaline phosphates (Nemet et al., 2002) increased bone and body mass as determined by dual-energy-x-ray absorptiometry (Moyer-Mileur et al., 2000), and prevented bone strength deterioration as determined by bone speed of sound (SOS) measurements (Litmanovitz, Dolfin, & Friedland, 2003).
Inasmuch as our massage therapy protocol also involves passive movement of the limbs that is similar to the exercise protocol used in the bone growth studies, the increase in serum bone formation marker observed following exercise may also occur following massage therapy. This would be true especially because massage therapy leads to increased activity (Scafidi, Field, Schanberg, Bauer & Vega-Lahr, 1986). Preterm infant bone growth following passive movements or exercise of the limbs may be mediated by elevated IGF-1. IGF-1 levels play a critical role in the formation, maintenance and regeneration of bone mass (Yakar & Rosen, 2003).
Research on ways of Delivering MassageTherapy/Exercise
Other research in the area of preterm infant massage therapy has focused on the delivery of massage therapy protocols. This research includes studies on mothers or parents as the therapists, on the use of oils to enhance the therapy effects and on hospital cost savings.
Using Mothers As the Therapists
At least one study has documented equivalent effects of professionals and mothers performing the preterm infant massages (Goldstein-Ferber et al, 2002). The Goldstein-Ferber et al (2002) study replicated the results of increased weight gain following massage therapy by both mothers and professionals. In this study, preterm infants were assigned to three groups including one treatment group in which the mothers performed the massage and another in which professionals unrelated to the infant administered the treatment. These two groups were then compared to a control group. Over the 10-day study period, the two treatment groups gained significantly more weight compared to the control group suggesting that mothers were able to achieve the same effect as that of trained professionals. In addition, the mothers who massaged their infants in this study experienced a decrease in depression symptoms, which are often seen in mothers of preterm infants. In our study using mothers as the massage therapists, even one session was effective in lowering both the mothers' depression and anxiety symptoms (Feijo, Hernandez-Reif, Field, Burns, Valley-Gray & Simco, 2006).
Oil Enhances Massage Therapy Effects
Oil massage for newborns is reported to improve weight gain by better thermoregulation. Transcutaneous absorption has also been suggested as a possible mechanism. A recent study compared the effects of massage with coconut oil versus mineral oil and placebo (powder) on growth velocity and behavior in preterm infants (Sankaranarayanan, Mondkar, Chauhan, Mascarenhas, Mainkar & Salvi, 2005). Preterm infants were randomized to receive massage with either coconut oil, mineral oil or powder. Oil massage was given by a trained person four times a day until discharge and thereafter by the mother until 31 days of age. Coconut oil massage resulted in significantly greater weight gain velocity as compared to mineral oil and powder in the preterm infants' group. The preterm infants receiving coconut oil massage also showed a greater length gain velocity compared to the powder group.
A similar study compared the effects of essential fatty acid (EFA) rich-safflower oil and saturated fat rich coconut oil on the fatty acid profiles of massaged infants (Solanki, Matnani, Kalem Joshi, Bavdekar, Bhave & Pandit, 2005). The NICU infants were randomly assigned to three oil groups; 1) safflower oil; 2) coconut oil; and 3) no oil controls. In each group, the infants were massaged four times a day for five days under controlled temperature and feeding conditions. Pre and post oil massage blood samples were analyzed for triglycerides and fatty acid profiles using gas chromatography. Post oil triglyceride values were significantly increased in both oil groups and also in the control group. However, the increase was significantly greater in the oil groups as compared to the control group. Fatty acid profiles (gas chromatography) suggested a significant increase in EFAs (linoleic acid and arachidonic acid) in the safflower oil group and saturated fats in the coconut oil group. This study showed that topically applied oil could be absorbed in neonates and is probably available for nutritional purposes. The fatty acid constituents of the oil can influence the changes in the fatty acid profiles of the massaged babies.
Even massage with synthetic oil has positive effects. It is also less likely than natural oils to lead to an allergic reaction. In a study we conducted, massage with oil was compared to massage without oil (Field, Schanberg, Davalos, & Malphurs, 1996). As can be seen in table 3, those infants who were massaged with oil showed less motor activity, less averting behavior (grimacing and head turning), less stress behavior (mouthing and clenched fists), a greater increase in vagal activity and a greater decrease in saliva cortisol levels (see table 3).
Table 3.
Means for behaviors and vagal tone and cortisol change in massage with Oil and massage with No Oil.
| Massage | |||
|---|---|---|---|
| Variables | Oil | No oil | p level |
| Motor activity (% time) | 45.00 | 56.00 | .05 |
| Averting behaviors | |||
| grimacing | 2.20 | 3.30 | .05 |
| head turning | 1.40 | 2.60 | .05 |
| Stress behaviors | |||
| mouthing | 1.80 | 5.90 | .05 |
| clenched fists | 3.70 | 9.20 | .01 |
| Vagal tone change | +.50 | +.20 | .05 |
| Cortisol (ng/nl) change | -.98 | -.03 | .05 |
Hospital Cost Savings
The greater weight gain documented by several investigators is associated with 3-6 days shorter hospital stays. A recent cost-benefit analysis suggested a hospital cost savings of approximately $10,000 per infant (or 4.7 billion dollars across the 470,000 preterm infants born each year) (Field, Hernandez-Reif & Freedman, 2004). Despite these benefits, a recent survey revealed that only 38% of NICUs offer infant massage or instruction to parents in infant massage (Field et al., 2004). The same 84 neonatologists polled in this survey suggested that preterm infant massage would not be widely adopted until underlying mechanisms are known.
Potential Underlying Mechanisms for the Effects of Massage Therapy
Some potential underlying mechanisms have been examined for the effects of massage therapy on preterm infant weight gain. Increased calorie consumption and/or greater calorie conservation was first explored as a potential mediator of the effects of massage therapy on weight gain. However, findings across our studies consistently showed that preterm infants receiving massage therapy did not consume more calories (Diego et al., 2005; Dieter, et al., 2003; Field et al, 1986; Scafidi et al, 1990; Wheeden et al, 1993). Also, contrary to our energy savings model (i.e. less activity leading to less calorie expenditure), the massaged infants spent more time being active than the control infants and, nonetheless, they gained more weight (Dieter, et al., 2003; Scafidi et al, 1986; Scafidi et al, 1990) (see Table 1).
In our recent model, we suggested that massage therapy led to weight gain via increased vagal activity, which, in turn, stimulated gastric motility. Increased vagal activity is supported by our recent finding that massage therapy with moderate pressure versus light pressure (SHAM) versus standard care (control) leads to increased heart rate variability, a marker of vagal activity (see Figure 1) (Diego et al., 2005). Vagal activity during massage therapy was significantly related to weight gain (r = .66, p < .01) Gastric motility (EEG) increased in the same study and was significantly related to weight gain (r= .55, p < .01) (Figure 1) (Diego et al., 2005). Taken together, these findings suggest that moderate pressure massage therapy leads to increased gastric motility and weight gain via increased vagal activity.
Figure 1.

Trend Analyses on Vagal Tone (high frequency component of heart rate variability) and Gastric Motility (2-4 cpm EGG) 15-minutes before, during and after treatment (error bars denote +- 2 SE) in massage (moderate pressure), sham (light pressure) and control groups. Preterm infants who received massage therapy exhibited increased HF during the massage (F (1,15)=4.54, p<.05, quadratic trend for massage group only) and increased gastric activity following the massage (F (1,15)=10.66, p<.01, linear trend for massage group only).
In a study to determine whether preterm infant massage leads to consistent increases in vagal activity and greater weight gain, EKG and EGG were recorded in 80 preterm infants randomly assigned to a moderate pressure massage therapy group or to a standard care control group to assess vagal activity and gastric motility responses to massage therapy (Diego, Field, Hernandez-Reif, Deeds, Ascencio & Begert, 2006). The massaged infants exhibited consistent increases in vagal activity and gastric motility on both the first and the last days of the 5-day study, and these increases were, in turn, associated with weight gain during the 5-day treatment period (see Figure 2).
Figure 2.

Mean vagal activity and gastric motility on the first and last days of the study for preterm infants assigned to the control (closed circles) and massage group (open circles).
Moderate Pressure is Critical
Moderate pressure may be an essential component of the infant massage, as a recent study by our group revealed that preterm infants who received moderate pressure stroking gained significantly more weight (26% more) than infants who received light pressure stroking (Diego et al., 2005) (see table 1). Similarly, static, light pressure touch does not result in greater weight gain as reported by others including the Cochrane Review based on the compilation of several data bases (Harrison, Williams, Berbaum, Stem & Leeper, 2000; Vickers et al., 2004).
Moderate pressure massage also leads to more organized behavior. In a replication study by our group, sixty-eight preterm infants were randomly assigned to a moderate or to a light pressure massage therapy group to receive 15 minute massages 3 times per day for 5 days (Field, Diego, Hernandez-Reif, Deeds & Figuereido, 2006). Behavior state, stress behaviors and heart rate were recorded for 15 minutes before and during the first 15-minute therapy session. Weight gain was recorded over the 5 day therapy period. The moderate versus light pressure massage group gained significantly more weight per day (see Table 4). During the behavior observations the moderate versus light pressure massage group showed significantly lower increases from the pre-session to the session recording on: 1) active sleep; 2) fussing; 3) crying; 4) movement; and 5) stress behavior (hiccupping) (see Table 4). They also showed a smaller decrease in deep sleep, a greater decrease in heart rate and a greater increase in vagal tone. Thus, the moderate pressure massage therapy group appeared to be more relaxed and less aroused than the light pressure massage group which may have contributed to the greater weight gain of the moderate pressure massage therapy group. Similar data were reported on another sample. Stress behavior and movement were diminished in the massage group by the last day of the study (Hernandez-Reif, Diego & Field, 2007) (see figure 3) Moderate pressure was also used in this study.
Table 4.
Means for neonatal measures for moderate and light pressure massage therapy groups pre and during therapy.
| Groups | ||||
|---|---|---|---|---|
| Moderate | Light | |||
| Pre | During | Pre | During | |
| Weight gain (g) | 22.2 | 27.8* | 28.8 | 27.4 |
| During sleep (% time) | 38.9 | 35.9 | 34.5 | 7.9* |
| Fussing (% time) | 0.1 | 0.2 | 0.0 | 16.0* |
| Crying (% time) | 0.6 | 0.7 | 1.8 | 11.6* |
| Movement (% time) | 6.9 | 6.1 | 9.9 | 18.0* |
| Hiccuping (% time) | 1.6 | 2.6 | 2.9 | 7.7** |
| Heart rate (BPM) | 171.1 | 164.6* | 168.0 | 168.7 |
p<05.
p<.01.
Figure 3.
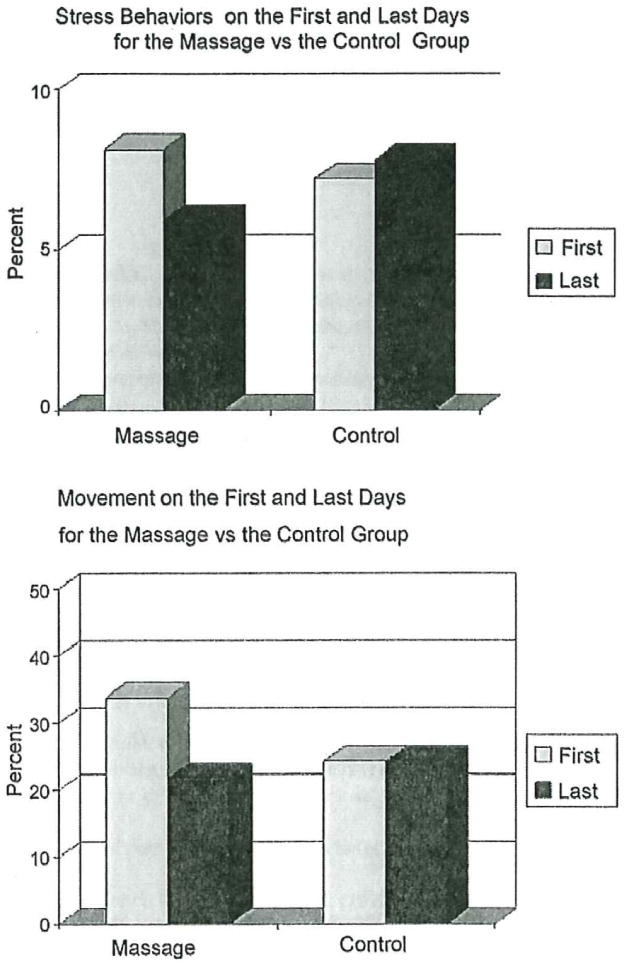
Stress behaviors on the first and last days for the massage vs. the control group. Movement on the first and last days for the massage vs. the control group.
In our study, moderate pressure, but not light pressure massage increased vagal activity (high frequency component (HF) of heart rate variability) (HRV) (Diego et al., 2005), suggesting that the stimulation of pressure receptors increases vagal activity. In that study, only those infants who exhibited increased vagal activity exhibited greater weight gain. Although many tactile stimulation studies have been conducted with preterm infants, only those that involved moderate pressure massage resulted in greater weight gain (Diego et al., 2005; Field et al., 1986; Scafidi et al, 1990), suggesting that it is the stimulation of pressure receptors that mediates the effects of massage therapy on enhanced vagal activity, gastric motility and weight gain.
Data analyses conducted on a larger sample revealed the following (see figure 4 and tables 5 and 6) (Diego et al, 2007). Massage therapy explained 19% of the variance in the change in vagal activity, leaving at least 81% of the variance “unaccounted for” in the vagal tone change. This could be due to other factors such as stimulant use in preemie care or the fact that we dummy coded massage as yes or no versus using it as a continuous variable; 2) the amount of change in vagal activity, in turn, explained 41% of the variance in the change in gastric motility observed during the massage period; 3) the change in calorie consumption during the study period was not related to whether infants received massage therapy or not. However, the change in calorie consumption during the treatment period explained at least 9% of the variance in weight gain during the treatment period; 4) the model supports a pathway where massage therapy leads to vagal activity, which, in turn, leads to weight gain. However, the effects of vagal activity on weight gain are only partially mediated by the change in gastric activity, as vagal activity contributed to at least 4% of the variance in weight gain independent of gastric motility. This might be explained by the vagus branching to other areas that may have contributed to the weight gain including the pancreas (insulin release) and HPA axis (decreased cortisol); and 5) the final model only explained 28% of the variance in preterm infant weight gain which in part relates to the fact that not all infants who received massage gained more weight. Also, other variables we did not measure would likely contribute to the variance. These include increased activity and increased IGF-1, which we have seen in our massage groups.
Figure 4.
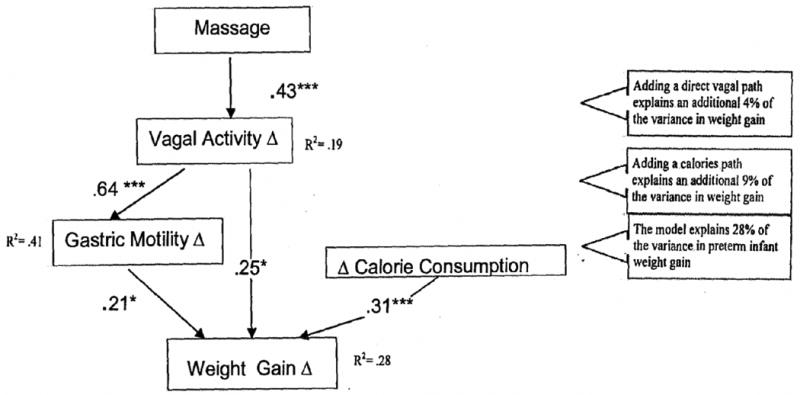
A preliminary path analysis entering potential mediating variables for the massage therapy/ weight gain relationship.
Corrected Model, Chi2 (5)= 6.96, p=.98
Table 5.
Mean changes (Δ) in weight gain, vagal activity, gastric motility and kilocalories.
| Control (N=38) | Massage (N=44) | F | p | |
|---|---|---|---|---|
| ΔWeight Gain (g/kg/day) | -.25 (1.20) | .37 (.90) | 7.17 | p<01 |
| ΔVagal Activity | -.03 (.29) | .43 (.61) | 18.23 | p<01 |
| ΔGastric Motility | .02 (.89) | 1.67 (1.65) | 8.67 | p<.01 |
| ΔKilocalories | 2.90 (9.9) | 3.74 (10.25) | .14 | N.S. |
Table 6.
Correlation analysis for changes in weight gain, vagal activity, gastric motility and kilocalories.
| Massage | Weight Gain | Vagal Activity G | astric Motility | |
|---|---|---|---|---|
| ΔWeight Gain (g/kg/day) | r = .23, p<.05 | |||
| ΔVagal Activity | r = .43, p<.01 | r = .40, p<.01 | ||
| ΔGastric Motility | r = .31, p<.01 | r = .39, p<.01 | r = .64, p<.01 | |
| ΔKilocalories | r = .04, N.S. | r = .33, p<.01 | r = .05, N.S. | r = .05, N.S. |
Our hypothesized massage therapy model is supported by several lines of evidence. For example, anatomical studies indicate that baroreceptors and, to a lesser extent, mechanoreceptors within the dermis (i.e. Pacinian corpuscles) are innervated by vagal afferent fibers projecting to the vagal nucleus of the solitary tract (NTS), the predominant source of afferent inputs to the efferent neurons of the nucleus ambiguous (NA) and the dorsal motor nucleus of the vagus (DMN) (Kandel, Schwartz & Jessell, 2000). The DMN, in turn, gives rise to most of the efferent fibers that provide parasympathetic control of the gastro-intestinal system in the form of the gastric (stomach, proximal duodenum), hepatic (liver) and celiac (pancreas, spleen, kidneys) branches of the vagus (Chang, Mashimo & Goyal, 2003; Kandel et al., 2000).
Direct stimulation of the vagus nerve can regulate gastric motility, can enhance food digestion and can increase the availability of nutrients (Chang et al., 2003). Greater nutrient availability can, in turn, increase IGF-1 levels (Thissen, Ketelslegers & Underwood, 1994). Vagal stimulation also promotes the release of insulin (Rozman, Bunc & Zorko, 2004), and insulin has been shown to stimulate the synthesis and release of IGF-1 (Kalme, Loukovaara, Koistinen, Koistinen, Seppala & Leinonen, 2001; Thissen et al., 1994). The stimulation of pressure receptors can also promote the release of insulin (Marchini, Lagercrantz, Feuerberg, Winberg, Uvnas-Moberg, 1987). Taken together, these findings suggest that stimulation of pressure receptors (as in massage) increases vagal activity, and vagal stimulation facilitates the release of insulin and indirectly leads to the release of IGF-1. Insulin-like-growth-factor-I (IGF-1) plays a key role in regulating preterm infant growth. IGF-1 is strongly correlated with placental weight, birthweight, body length and Ponderal Index (Colonna, Pahor, de Vonderweid, Tonini & Radillo, 1996; Klauwer, Blum, Hanitsch, Rascher, Lee & Kiess, 1997; Leger, Oury, Noel, Baron, Benali, Blot & Czernichow, 1996; Osorio, Torres, Moya, Pezzullo, Salafia, Baxter, Schwander & Fant, 1996), and can significantly predict growth velocity in preterm infants (Kajantie, Dunkel, Rutane, Seppala, Koistinen & Sarnesto, 2002).
Both insulin and IGF-1 were noted to increase in a recent study we conducted using massage therapy with preterm infants (Field et al, in review). In that study preterm neonates were randomly assigned to massage therapy or a standard treatment control group. Despite similar formula intake, the massaged preterm neonates showed greater increases during the 5 day period in: 1) weight gain; 2) serum levels of insulin; and 3) insulin-like growth factor-1 (IGF-1) (see figure 5). Increased weight gain was significantly correlated with insulin and IGF-1.
Figure 5.
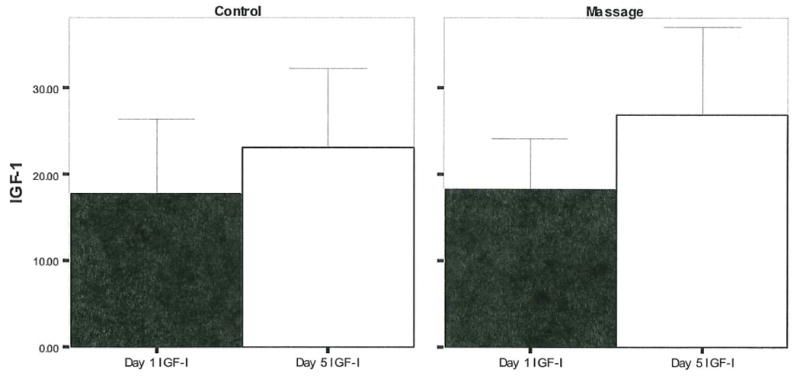
IGF-1 levels increased from day 1 to day 5 for infants assigned to the moderate massage therapy (t (20) = 2.25, p < .05) but not the standard care control group (t (20) = 1.65, N.S.).
Summary
In this paper, preterm infant massage therapy studies are reviewed. Massage therapy has led to weight gain in preterm infants when moderate pressure massage was provided. In studies on passive movement of the limbs, preterm infants also gained significantly more weight, and their bone density also increased. Research on ways of delivering the massage is also explored including using mothers versus therapists and the added effects of using oils. The use of mothers as therapists was effective in at least one study. The use of oils including coconut oil and safflower oil enhanced the average weight gain, and the transcutaneous absorption of oil also increased triglycerides. In addition, the use of synthetic oil increased vagal activity, which may indirectly contribute to weight gain. The weight gain was associated with shorter hospital stays and, thereby, significant hospital cost savings. Despite these benefits, preterm infant massage is only practiced in 38% of neonatal intensive care units. This may relate to the underlying mechanisms not being well understood. The increases noted in vagal activity, gastric motility, insulin and IGF-1 levels following moderate pressure massage are potential underlying mechanisms. However, those variables combined do not explain all of the variance in weight gain, highlighting the need for additional mechanism studies.
Acknowledgments
We would like to thank the mothers and infants who participated in our studies which were supported by NIH Senior Research Scientist Awards (# MH 00331 and # AT 01585) and an NIMH Merit award (MH # 46586) to Tiffany Field and funding from Johnson and Johnson Pediatric Institute.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Backstrom M, Kuusela A, Maki R. Metabolic bone disease of prematurity. Annuals of Medicine. 1996;28:275–82. doi: 10.3109/07853899608999080. [DOI] [PubMed] [Google Scholar]
- Chang HY, Mashimo H, Goyal RK. Musings on the wanderer: what's new in our understanding of vago-vagal reflex? IV. Current concepts of vagal efferent projections to the gut. American Journal of Physiology Gastrointestinal and Liver Physiology. 2003;284:G357–66. doi: 10.1152/ajpgi.00478.2002. [DOI] [PubMed] [Google Scholar]
- Cifra HL, Sancho MN. Massage therapy with preterm infants and children with chronic illnesses. In: Field T, editor. Touch and Massage Therapy in Early Development. Johnson & Johnson Pediatric Institute, L.L.C.; 2004. [Google Scholar]
- Colonna F, Pahor T, de Vonderweid U, Tonini G, Radillo L. Serum insulin-like growth factor-I (IGF-I) and IGF binding protein-3 (IGFBP-3) in growing preterm infants on enteral nutrition. Journal of Pediatric Endocrinology and Metabolism. 1996;9:483–489. doi: 10.1515/jpem.1996.9.4.483. [DOI] [PubMed] [Google Scholar]
- De-Roiste A, Bushnell IWR. Tactile stimulation: short and long-term benefits for preterm infants. British Journal of Developmental Psychology. 1996;41:41–53. [Google Scholar]
- Diego M, Field T, Hernandez-Reif M. Vagal activity, gastric motility, and weight gain in massaged preterm neonates. The Journal of Pediatrics. 2005;147:50–55. doi: 10.1016/j.jpeds.2005.02.023. [DOI] [PubMed] [Google Scholar]
- Diego MA, Field T, Hernandez-Reif M, Deeds O, Ascencio A, Begert G. Preterm infant massage elicits consistent increases in vagal activity and gastric motility that are associated with greater weight gain. Acta Pediatrica. 2006;21:1588–91. doi: 10.1111/j.1651-2227.2007.00476.x. [DOI] [PubMed] [Google Scholar]
- Dieter JN, Field T, Hernandez-Reif M, Emory EK, Redzepi M. Stable preterm infants gain more weight and sleep less after five days of massage therapy. Journal of Pediatric Psychology. 2003;28:403–11. doi: 10.1093/jpepsy/jsg030. [DOI] [PubMed] [Google Scholar]
- Duan L, Li W, Shi F. Studying impact of touching on growth and development of infants. Chinese Nursing Research. 2002;16:5. [Google Scholar]
- Eliakim A, Nemet D, Friedland O, Dolfin T, Regev R. Spontaneous activity in premature infants affects bone strength. Journal of Perinatology. 2002;22:650–2. doi: 10.1038/sj.jp.7210820. [DOI] [PubMed] [Google Scholar]
- Feijo L, Hernandez-Reif M, Field T, Burns W, Valley-Gray S, Simco E. Mothers' depressed mood and anxiety levels are reduced after massaging their preterm infants. Infant Behavior and Development. 2006;29:476–80. doi: 10.1016/j.infbeh.2006.02.003. [DOI] [PubMed] [Google Scholar]
- Field T, Diego M, Hernandez-Reif M, Dieter J, Kumar A, Schanberg S, Kuhn C. Insulin and Insulin-Like Growth Factor I (IGF-1) Increase in Preterm Infants Following Massage Therapy. Pediatrics In Review. [Google Scholar]
- Field T, Diego MA, Hernandez-Reif M, Deeds O, Figuereido B. Moderate versus light pressure massage therapy leads to greater weight gain in preterm infants. Infant Behavior and Development. 2006;29:574–8. doi: 10.1016/j.infbeh.2006.07.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Field T, Hernandez-Reif M, Freedman J. Stimulation programs for preterm infants. Social Policy Report. 2004;18:1–19. [Google Scholar]
- Field T, Schanberg S, Davalos M, Malphurs J. Massage with oil has more positive effects on newborn infants. Pre and Perinatal Psychology Journal. 1996;11:73–78. [Google Scholar]
- Field T, Schanberg SM, Scafidi F, Bauer CR, Vega-Lahr N, et al. Tactile/kinesthetic stimulation effects on preterm neonates. Pediatrics. 1986;77:654–658. [PubMed] [Google Scholar]
- Goldstein-Ferber S, Kuint J, Weller A, Feldman R, Dollberg S, Arbel E, Kohelet D. Massage therapy by mothers and trained professionals enhances weight gain in preterm infants. Early Human Development. 2002;67:37–45. doi: 10.1016/s0378-3782(01)00249-3. [DOI] [PubMed] [Google Scholar]
- Harrison LL, Williams AK, Berbaum ML, Stem JT, Leeper J. Physiologic and behavioral effects of gentle human touch on preterm infants. Research in Nursing & Health. 2000;23:435–446. doi: 10.1002/1098-240X(200012)23:6<435::AID-NUR3>3.0.CO;2-P. [DOI] [PubMed] [Google Scholar]
- Hernandez-Reif M, Diego M, Field T. Preterm infants show reduced stress behaviors and activity after 5 days of massage therapy. Infant Behavior & Development. 2007;30:557–61. doi: 10.1016/j.infbeh.2007.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kajantie E, Dunkel L, Rutanen EM, Seppala M, Koistinen R, Sarnesto A, Andersson S. IGF-I, IGF binding protein (IGFBP)-3, phosphoisoforms of IGFBP-1, and postnatal growth in very low birth weight infants. The Journal of Clinical Endocrinology and Metabolism. 2002;87:2171–2179. doi: 10.1210/jcem.87.5.8457. [DOI] [PubMed] [Google Scholar]
- Kalme T, Loukovaara M, Koistinen H, Koistinen R, Seppala M, Leinonen P. Factors regulating insulin-like growth factor binding protein-3 secretion from human hepatoma (HepG2) cells. The Journal of Steroid Biochemistry and Molecular Biology. 2001;78:131–135. doi: 10.1016/s0960-0760(01)00089-9. [DOI] [PubMed] [Google Scholar]
- Kandel E, Schwartz J, Jessell T. Principles in Neural Science. 4th. McGraw Hill; New York: 2000. [Google Scholar]
- Ke G, Ling X, Li L. Clinical survey of improved massage method developing infants' growth and development. China Nurse. 2001;36:278–280. [Google Scholar]
- Klauwer D, Blum WF, Hanitsch S, Rascher W, Lee PD, Kiess W. IGF-I, IGF-II, free IGF-I and IGFBP-1, -2 and -3 levels in venous cord blood: relationship to birth weight, length and gestational age in healthy newborns. Acta Paediatrica. 1997;86:826–833. doi: 10.1111/j.1651-2227.1997.tb08605.x. [DOI] [PubMed] [Google Scholar]
- Leger J, Oury JF, Noel M, Baron S, Benali K, Blot P, Czernichow P. Growth factors and intrauterine growth retardation. I. Serum growth hormone, insulin-like growth factor (IGF)-I, IGF-II, and IGF binding protein 3 levels in normally grown and growth-retarded human fetuses during the second half of gestation. Pediatrics Research. 1996;40:94–100. doi: 10.1203/00006450-199607000-00017. [DOI] [PubMed] [Google Scholar]
- Litamanovitz I, Dolfin T, Friedland O, et al. Early physical activity intervention prevents decrease of bone strength in very low birth weight infants. Pediatrics. 2003;112:15–19. doi: 10.1542/peds.112.1.15. [DOI] [PubMed] [Google Scholar]
- Liu DY. Clinical experience in infant massage : 100 case studies. Chongqing Medicine. 2005;34:301. [Google Scholar]
- Liu ChunLi. The effect of touching on healthy infants' weight. Journal of Huaihai Medicine. 2005;23:137. [Google Scholar]
- Lu Jiao, Li Ju Zhan, Wu Li Fang. A study of the effect of touch on health in infants. Practical Clinical Medicine. 2005;6:119–121. [Google Scholar]
- Marchini G, Lagercrantz H, Feuerberg Y, Winberg J, Uvnas-Moberg K. The effect of non-nutritive sucking on plasma insulin, gastrin, and somatostatin levels in infants. Acta Paediatrica Scandinavica. 1987;76:573–578. doi: 10.1111/j.1651-2227.1987.tb10523.x. [DOI] [PubMed] [Google Scholar]
- Mathai S, Fernandez A, Mondkar J, Kanbur W. Effects of tactile-kinesthetic stimulation in preterms: a controlled trial. Indian Pediatrics. 2001;38:1091–1098. [PubMed] [Google Scholar]
- Moyer-Mileur LJ, Brunstetter V, McNaught TP, Gill G, Chan GM. Daily physical activity program increases bone mineralization and growth in preterm very low birth weight infants. Pediatrics. 2000;106:1088–92. doi: 10.1542/peds.106.5.1088. [DOI] [PubMed] [Google Scholar]
- Moyer-Mileur L, Luetkemeier M, Boomer L, Chan G. Effects of physical activity on bone mineralization in premature infants. Journal of Pediatrics. 1995;127:620–5. doi: 10.1016/s0022-3476(95)70127-3. [DOI] [PubMed] [Google Scholar]
- Myburgh KH. Exercise and peak bone mass: an update. South African Journal of Sports Medicine. 1998;5:3–9. [Google Scholar]
- Na Zhuo Hua, Xie Hui Yun, Huang Jian Hua. The effect of infant massage on growth. New Journal of Traditional Chinese Medicine. 2005;37:69–70. [Google Scholar]
- National Center for Health Statistics. Health. United States: 2005. 2007. [Google Scholar]
- Nemet D, Dolfin T, Litmanowitz I, Shainkin-Kestenbaum R, Lis M, Eliakim A. Evidence for exercise-induced bone formation in premature infants. International Journal of Sports Medicine. 2002;23:82–85. doi: 10.1055/s-2002-20134. [DOI] [PubMed] [Google Scholar]
- Osorio M, Torres J, Moya F, Pezzullo J, Salafia C, Baxter R, Schwander J, Fant M. Insulin-like growth factors (IGFs) and IGF binding proteins- 1, -2, and -3 in newborn serum: relationships to fetoplacental growth at term. Early Human Development. 1996;46:15–26. doi: 10.1016/0378-3782(96)01737-9. [DOI] [PubMed] [Google Scholar]
- Rigo J, De Curtis M, Pieltain C, Picaud JC, Salle BL, Senterre J. Bone mineral metabolism in the micropremie. Clinics in Perinatology. 2000;27:147–170. doi: 10.1016/s0095-5108(05)70011-7. [DOI] [PubMed] [Google Scholar]
- Rodriguez JI, Garcia-Alix A, Palacios J, Paniagua R. Changes in the long bones due to fetal immobility caused by neuromuscular disease: a radiographic and histological study. Journal of Bone and Joint Surgery: American Volume. 1988;70:1052–1060. [PubMed] [Google Scholar]
- Rozman J, Bunc M, Zorko B. Modulation of hormone secretion by functional electrical stimulation of the intact and incompletely dysfunctional dog pancreas. Brazilian Journal of Medical and Biological Research. 2004;37:363–70. doi: 10.1590/s0100-879x2004000300012. [DOI] [PubMed] [Google Scholar]
- Sankaranarayanan K, Mondkar JA, Chauhan MM, Mascarenhas BM, Mainkar AR, Salvi RY. Oil massage in neonates: an open randomized controlled study of coconut versus mineral oil. Indian Pediatrics. 2005;42:877–84. [PubMed] [Google Scholar]
- Scafidi F, Field TM, Schanberg SM, Bauer CR, Tucci K. Massage stimulates growth in preterm infants: A replication. Infant Behavior and Development. 1990;13:167–188. [Google Scholar]
- Scafidi F, Field TM, Schanberg SM, Bauer C, Vega-Lahr N, et al. Effects of tactile/kinesthetic stimulation on the clinical course and sleep/wake behavior of preterm neonates. Infant Behavior and Development. 1986;9:91–105. [Google Scholar]
- Shi Li, Xue Li Rong. The clinical observation of touching towards the neonatal health's affection. Journal of Henan University. 2002;21:26–27. [Google Scholar]
- Solanki K, Matnani M, Kale M, Joshi K, Bavdekar A, Bhave S, Pandit A. Transcutaneous absorption of topically massaged oil in neonates. Indian Pediatrics. 2005;42:998–1005. [PubMed] [Google Scholar]
- Sun Hai Yun, Gao Xiang Yu, Zhao Xue Mei. A comparative study on influence of touching on growth, development and jaundice of normal infants. Chinese Nursing Research. 2004;18:1468–1469. [Google Scholar]
- Thissen JP, Ketelslegers JM, Underwood LE. Nutritional regulation of the insulin-like growth factors. Endocrinology Review. 1994;15:80–101. doi: 10.1210/edrv-15-1-80. [DOI] [PubMed] [Google Scholar]
- Vickers A, Ohlsson A, Lacy JB, Horsley A. Massage for promoting growth and development of preterm and/or low birth-weight infants. Cochrane Database System Review. 2004;2:CD000390. doi: 10.1002/14651858.CD000390.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wheeden A, Scafidi FA, Field T, Ironson G, Valdeon C, et al. Massage effects on cocaine-exposed preterm neonates. Developmental and Behavioral Pediatrics. 1993;14:318–322. [PubMed] [Google Scholar]
- Yakar S, Rosen CJ. From mouse to man: Redefining the role of insulin-like growth factor-I in the acquisition of bone mass. Experimental Biology and Medicine. 2003;228:245–52. doi: 10.1177/153537020322800302. [DOI] [PubMed] [Google Scholar]
- Zhai J, Pan Xian R, Hua JR. The effect of massage on growth: a clinical study. Journal of Sichuan continuing Education College of Public Health and Managerial Sciences. 2001;20:23. [Google Scholar]