

Abstract
Background:
Nitric oxide (NO) production following bacterial infection may play a physiological role in the host defense mechanism due to its antimicrobial activity. However, excess production of NO in severe infection such as sepsis has been implicated in the pathogenesis of septic shock. To determine whether a nitronyl nitroxide NO scavenger compound could prevent the hemodynamic and blood gas alterations in sepsis, bacterial lipopolysaccharide (LPS: 250ng/kg/min) was administered for 2 h in anesthetized dogs with or without infusion of carboxy-2-phenyl-4, 4, 5, 5-tetramethylimidazoline-1-oxyl-3-oxide (carboxy-PTIO: 0.1 mg/kg/min) for 1 h. Control animals received isotonic saline instead of LPS with or without carboxy-PTIO.
Results:
Infusion of LPS caused a marked decrease in mean arterial pressure (MAP), metabolic acidosis, and hypoxia. These effects were reversed by co-administration of carboxy-PTIO, without affecting other hemodynamic parameters. In control animals, neither hemodynamic nor blood gas parameters changed with or without carboxy-PTIO.
Conclusion:
These results indicate that carboxy-PTIO attenuates LPS-induced hypotension, metabolic acidosis, and hypoxia by scavenging excess NO from the circulation without affecting NO synthase (NOS) activity. An NO scavenger, carboxy-PTIO, may be preferable to non-selective NOS inhibitors for the treatment of human septic shock.
Keywords: carboxy-PTIO, hemodynamics, lipopolysaccharide, nitric oxide, septic shock
Introduction
Nitric oxide production by activated macrophages following infection may play a physiological role in the host defense mechanism due to its antimicrobial activity [1,2]. However, sustained and excessive production of NO in severe infection such as sepsis has been implicated in the pathogenesis of septic shock [3,4,5]. Septic shock is characterized by a hyperdynamic state (hypotension, tachycardia, normal or increased cardiac output associated with low systemic vascular resistance), an impairment of tissue perfusion, and hyporesponsiveness to vasoconstrictors [6]. Nitric oxide is produced by three distinct isoenzymes termed NO synthases (NOS): brain and endothelial constitutive NOS (cNOS), and inducible NOS (iNOS). Nitric oxide synthesized by endothelial cNOS is involved in the regulation of basal vascular tone and anti-thrombotic effect by inhibiting platelet aggregation and leukocyte adhesion to the endothelial surface [1]. Excess production of NO by iNOS, stimulated by bacterial lipopolysaccharide (LPS) and several cytokines, may contribute to the cardiovascular dysfunction seen in septic shock [3,4,5].
Several strategies can be used to reduce NO activity during septic shock. L-arginine analogues, such as NG-monomethyl-L-arginine (L-NMMA), NG-nitro-L-arginine (L-NNA), and NG-nitro-L-arginine methyl ester (L-NAME), are non-selective inhibitors for cNOS and iNOS [1,2]. Although these analogues increase blood pressure in septic shock models, they show various deleterious effects, such as decreasing cardiac output, oxygen delivery and metabolic acidosis [4,5,7], possibly due to the non-selective inhibition of endothelial cNOS as well as iNOS. To circumvent these deleterious effects by non-selective NOS inhibitors, relatively selective inhibitors for iNOS, such as aminoguanidine [8,9] and S-methylisothiourea [10], have been developed and studied in septic shock models. Other investigators have tested methylene blue, an inhibitor of soluble guanylate cyclase, which blocks the NO-mediated formation of cyclic guanosine monophosphate (cGMP), a second messenger for vasorelaxation in patients with septic shock [11].
Recently, Akaike et al [12] have reported that a nitronyl nitroxide compound, 2-phenyl-4, 4, 5, 5-tetramethylimidazoline-1-oxyl-3-oxide (PTIO) derivative, reacts with NO to generate NO2 and 2-phenyl-4, 4, 5, 5-tetramethylimidazoline-1-oxyl (PTI) derivative in a stoichiometric manner. Carboxy-PTIO, a water soluble derivative, has been shown to attenuate hypotension and renal dysfunction in LPS-treated rat models [13]. However, few studies have dealt with the detailed hemodynamic or metabolic effects of the novel NO scavenger in a septic shock dog model. In order to assess the therapeutic potential of carboxy-PTIO in human septic shock, our study was designed to examine the effects of carboxy-PTIO on hemodynamic and blood gas variables in LPS-induced septic shock dogs.
Materials and methods
Surgical preparation
The study was approved by the Institutional Review Board for the care of animal subjects, and the care and handling of the animals was in accord with National Institutes of Health guidelines. Twenty mongrel dogs, 12.6 ± 0.7 kg, were studied. The dogs were anesthetized for intubation with intravenous administration of pentobarbital (20 mg/kg), and connected to a ventilator. The inspired oxygen fraction was maintained at 0.3, and the ventilator rate and tidal volume were adjusted to obtain a normal arterial pH ad PCO2 using a pH/blood gas analyser (IL 1306A, Instrumentation Laboratory, Lexington, MA, USA). A catheter was inserted into the femoral vein and Ringer lactate solution (10 ml/kg/h) and pentobarbital (4 mg/kg/h) were administered throughout the study period. A pulmonary artery catheter (93A-141-7F, Baxter Healthcare Corp, Santa Ana, CA, USA) was inserted through the jugular vein. Another catheter was cannulated into the femoral artery for continuous measurement of systemic arterial pressure, and intermittent arterial blood sampling. Heart rate was monitored by electrocardiogram. After surgical preparation, the dogs were allowed to stabilize for 1 h.
LPS protocol
The dogs were divided into two experimental groups: in the LPS group (n = 7), LPS (0127:B8, Difco Detroit, MI, USA) was infused intravenously at a rate of 250 ng/kg/min for 2 h, as previously described [14]. In the LPS plus carboxy-PTIO group (n = 7), 30 min after the start of LPS administration (250 ng/kg/min, for 2 h), carboxy-PTIO (Dojindo Laboratories, Kumamoto, Japan) was infused at a rate of 0.1 mg/kg/min for 1 h.
Sham protocol
In sham-shocked dogs, isotonic saline instead of LPS was infused for 2 h without (sham-vehicle group n = 3) and with carboxy-PTIO (sham-carboxy-PTIO group, n = 3) for 1 h.
Measurements of hemodynamic and blood gas parameters
Heart rate (HR), mean arterial pressure (MAP), mean pulmonary arterial pressure (MPAP), pulmonary capillary wedge pressure (PCWP), and central venous pressure (CVP), were measured at baseline, 0.5, 1, 2, 3, and 4 h. Cardiac output was simultaneously measured at baseline, 1,2,3, and 4 h using the thermodilution technique with a cardiac output computer (9520A, Baxter Healthcare Corp, Santa Ana, CA, USA); the mean value of two measurements and the cardiac index (CI) were both calculated. Arterial and mixed venous blood gases were measured at baseline, 1, 2, 3, and 4 h. Systemic vascular resistance index (SVRI), pulmonary vascular resistance index (PVRI), oxygen delivery index (DO2I), and oxygen consumption index (VO2I) were calculated using standard formulae.
Statistical analysis
All data are presented as mean ± SEM. Parameters were compared over the study period using an analysis of variance for repeated measures. Where the F values was found to be significant, the data were compared with Turkey's test. Comparisons between the two groups at the same time point were analysed by one-way analysis of variance followed by Turkey's post hoc test when appropriate. P < 0.05 was considered statistically significant.
Results
Changes in hemodynamic parameters
In both the sham-vehicle group and the sham-carboxy-PTIO group, no significant hemodynamic changes occurred during the 4 h period (Fig 1a, and Table 1). In contrast, LPS administration caused a significant (P < 0.01) decrease in MAP during the 1-4 h period, and carboxy-PTIO reversed the LPS-induced hypotension (Fig 1b). After LPS administration, CI tended to decrease although not to a statistically significant degree, and SVRI did not change during the 4 h period (Fig 1b). Other hemodynamic parameters (PVRI, MPAP, PCWP, CVP) did not change during the 4 h period (Table 2).
Figure 1.
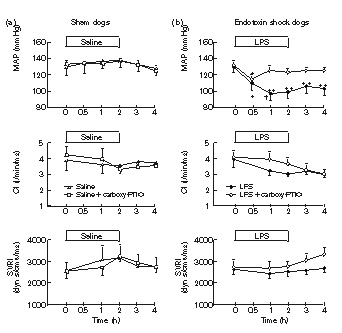
Changes in mean arterial pressure (MAP), cardiac index (CI), and systemic vascular resistance index (SVRI) in anesthetized dogs after 2 h intravenous administration of (a) isotonic saline or (b) bacterial lipopolysaccharide (LPS: 250 ng/kg/min) with or without 1 h infusion of carboxy-PTIO (0.1 mg/kg/min). Each point represents the mean of sham-vehicle group (n = 3), sham-carboxy-PTIO group (n = 3), LPS group (n = 7), and LPS plus carboxy-PTIO group (n = 7); bar shows SEM. *P < 0.05, **P < 0.01 vs baseline value. †P < 0.05; difference between the two groups at the same time point.
Table 1.
Hemodynamic and gas exchange parameters in anesthetized dogs after isotonic saline infusion with or without carboxy-PTIO
| Hours | |||||||
| Parameters | Treatment | 0 | 0.5 | 1 | 2 | 3 | 4 |
| HR (beats/min) | Saline | 145 ± 18 | 135 ± 18 | 128 ± 23 | 133 ± 18 | 143 ± 13 | 152 ± 15 |
| Carboxy-PTIO | 152 ± 14 | 153 ± 14 | 150 ± 11 | 157 ± 11 | 151 ± 8 | 155 ± 9 | |
| MPAP (mmHg) | Saline | 15 ± 2 | 15 ± 2 | 15 ± 2 | 15 ± 2 | 16 ± 1 | 16 ± 0 |
| Carboxy-PTIO | 16 ± 2 | 16 ± 1 | 15 ± 1 | 15 ± 1 | 16 ± 2 | 17 ± 2 | |
| PCWP (mmHg) | Saline | 7 ± 2 | 7 ± 2 | 6 ± 2 | 8 ± 3 | 7 ± 3 | 5 ± 1 |
| Carboxy-PTIO | 7 ± 1 | 7 ± 1 | 7 ± 1 | 8 ± 1 | 8 ± 1 | 8 ± 1 | |
| CVP (mmHg) | Saline | 4± 1 | 5 ± 0 | 5 ± 1 | 4 ± 1 | 4 ± 1 | 5 ± 0 |
| Carboxy-PTIO | 5 ± 1 | 5 ± 1 | 5 ± 1 | 5 ± 1 | 5 ± 1 | 5 ± 1 | |
| PVRI (dyn s/cm5m2) | Saline | 168 ± 5 | - | 176 ± 32 | 186 ± 27 | 214 ± 51 | 225 ± 57 |
| Carboxy-PTIO | 163 ± 10 | - | 164 ± 21 | 168 ± 17 | 175 ± 31 | 199 ± 31 | |
| DO2I (ml min/m2) | Saline | 701 ± 91 | - | 636 ± 122 | 608 ± 108 | 633 ± 103 | 632 ± 85 |
| Carboxy-PTIO | 705 ± 97 | - | 647 ± 78 | 535 ± 26 | 553 ± 12 | 575 ± 30 | |
| VO2I (ml min/m2) | Saline | 112 ± 7 | - | 116 ± 6 | 118 ± 11 | 121 ± 10 | 123 ± 9 |
| Carboxy-PTIO | 103 ± 8 | - | 114 ± 14 | 120 ± 3 | 132 ± 7 | 137 ± 8 | |
Values are mean ± SEM (n = 3). HR=heart rate; MPAP = mean pulmonary arterial pressure; PCWP = pulmonary capillary wedge pressure; CVP = central venous pressure; PVRI = pulmonary vascular resistance index; DO2I = O2 delivery index; VO2I, = O2 consumption index;- = not measured.
Table 2.
Hemodynamic and gas exchange parameters in anesthetized dogs after intravenous administration of bacterial lipopolysaccharide with or without carboxy-PTIO
| Hours | |||||||
| Parameters | Treatment | 0 | 0.5 | 1 | 2 | 3 | 4 |
| HR (beats/min) | LPS | 143 ± 18 | 144 ± 8 | 150 ± 11 | 152 ± 6 | 157 ± 8 | 155 ± 10 |
| Carboxy-PTIO | 144 ± 13 | 147 ± 12 | 154 ± 12 | 156 ± 11 | 155 ± 11 | 158 ± 12 | |
| MPAP (mmHg) | LPS | 17 ± 13 | 17 ± 13 | 16 ± 13 | 18 ± 4 | 18 ± 4 | 19 ± 5 |
| Carboxy-PTIO | 16 ± 1 | 16 ± 1 | 16 ± 1 | 17 ± 1 | 17 ± 1 | 17 ± 1 | |
| PCWP (mmHg) | LPS | 8 ± 2 | 7 ± 1 | 7 ± 2 | 7 ± 2 | 7 ± 2 | 8 ± 2 |
| Carboxy-PTIO | 8 ± 1 | 8 ± 1 | 8 ± 1 | 8 ± 1 | 9 ± 1 | 9 ± 1 | |
| CVP (mmHg) | LPS | 4 ± 1 | 4 ± 1 | 3 ± 1 | 3 ± 1 | 4 ± 1 | 5 ± 1 |
| Carboxy-PTIO | 4 ± 1 | 3 ± 1 | 4 ± 1 | 4 ± 1 | 5 ± 1 | 4 ± 1 | |
| PVRI (dyn s/cm5m2) | LPS | 180 ± 22 | - | 201 ± 17 | 270 ± 34 | 229 ± 35 | 252 ± 51 |
| Carboxy-PTIO | 157 ± 13 | - | 168 ± 11 | 177 ± 17 | 208 ± 17 | 229 ± 27 | |
| DO2I (ml min/m2) | LPS | 592 ± 59 | - | 538 ± 49 | 438 ± 43 | 482 ± 44 | 439 ± 35 |
| Carboxy-PTIO | 722 ± 83 | - | 725 ± 65 | 679 ± 64 | 616 ± 58 | 558 ± 50 | |
| VO2I (ml min/m2) | LPS | 128 ± 17 | - | 115 ± 12 | 117 ± 14 | 127 ± 18 | 124 ± 12 |
| Carboxy-PTIO | 125 ± 12 | - | 123 ± 12 | 120 ± 13 | 123 ± 16 | 130 ± 17 | |
Values are mean ± SEM (n = 7). LPS = lipopolysaccharide; HR = heart rate; MPAP = mean pulmonary arterial pressure; PCWP = pulmonary capillary wedge pressure; CVP = central venous pressure; PVRI = pulmonary vascular resistance index; DO2I = O2 delivery index; VO2I = O2 consumption index;- = not measured.
Changes in blood gas parameters
In both the sham-vehicle and the sham-carboxy-PTIO group, no appreciable changes in blood gas parameters (pH, PaO2, HCO3-, base excess) were observed during the 4 h period (Fig 2a). However, LPS administration caused metabolic acidosis and hypoxia, effects which were reversed by carboxy-PTIO (Fig 2b).
Figure 2.
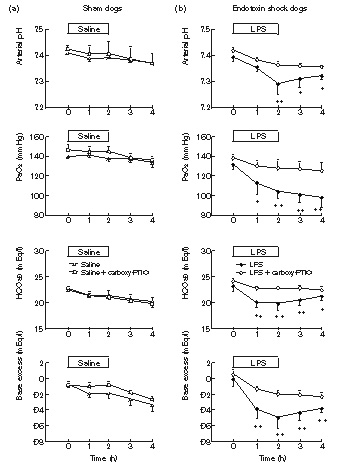
Changes in arterial pH, PaO2, HCO3-, and base excess in anesthetized dogs after 2 h intravenous administration of (a) isotonic saline or (b) bacterial lipopolysaccharide (LPS: 250 ng/kg/min) with or without 1 h infusion or carboxy-PTIO (0.1 mg/kg/min). Each point represents the mean of sham-vehicle group (n = 3), sham-carboxy-PTIO group (n = 3), LPS group (n = 7), and LPS plus carboxy-PTIO group (n = 7); bar shows SEM. *P < 0.05, **P < 0.01 vs baseline value.
Discussion
This study clearly demonstrates that infusion of carboxy-PTIO prevents LPS-induced hypotension as well as metabolic acidosis and hypoxia in an endotoxin shock dog model. In the present study, LPS caused a rapid (within 1 h) and sustained fall in MAP over a 4 h period. This early decrease in MAP may be partly caused by immediate NO release due to activation of endothelial cNOS. In fact, in a study by Szabó et al, LPS-treated rats experienced early (within 1 h) hypotension which was prevented by L-NAME, but early hyporeactivity to noradrenaline was not inhibited by dexamethasone, which blocks the induction of iNOS [15], suggesting that the early hypotension is probably due to NO generated by the activation of cNOS. The same group has further suggested that the early NO-related vascular changes may be associated with the formation of peroxynitrite from endothelial cNOS-derived NO and superoxide [16]. Taken together, the mechanism of LPS-induced hypotension is more likely due to NO-induced peripheral vasodilation and vascular injury by peroxynitrite.
In our study, LPS-induced hypotension was accompanied by a tendency towards decreased CI during the 4 h period, suggesting that cardiac dysfunction may be a contributing factor. As a result, the calculated SVRI did not decrease despite peripheral vasodilation. The cause of this phenomenon may be explained by the method of fluid resuscitation chosen for this study. Although 10 ml/kg/h crystalloid solution was administered during the study period, this fluid resuscitation might not be sufficient to produce high cardiac output as usually observed during human septic shock.
Carboxy-PTIO directly scavenges NO without affecting NOS activity [17]. Therefore, the antihypotensive action of carboxy-PTIO is most likely mediated through its reaction with NO [12] to eliminate excess NO in septic shock animal models. It has previously been reported that infusion of carboxy-PTIO (0.056–1.7 mg/kg/min for 1 h) into LPS-induced septic shock rats dose-despondently prevented the decrease in MAP and improved survival rate [13]. Therefore, we chose a lower carboxy-PTIO dose (0.1 mg/kg/min for 1 h) for our dog model. Although blood carboxy-PTIO levels gradually decrease after discontinuing infusion [13], the LPS-induced hypotension was completely prevented by the smaller dose of carboxyl-PTIO used in our study. Thus, continuous infusion of carboxy-PTIO for 1 h seems enough to maintain the plasma at a level high enough to scavenge excess NO in the circulation.
Administration of carboxy-PTIO did not increase SVRI or decrease CI during the 4 h period in our septic shock dog model. These findings are in contrast to a marked decrease in CI associated with peripheral vasoconstriction by non-selective NOS inhibitors, such as L-NMMA, L-NNA, and L-NAME [6,18,19]. It has been demonstrated that L-NMMA caused a reduction in coronary flow associated with a decrease in cardiac output in isolated rat hearts, possibly as a result of myocardial ischemia [20]. By contrast, it has recently been reported that carboxy-PTI, a reaction product of carboxy-PTIO and NO, has a potent vasodilator effect in the canine coronary artery without altering systemic hemodynamic variables [21]. This effect may be responsible for the maintenance of cardiac output following carboxy-PTIO administration, and may also contribute to the maintenance adequate regional blood flow.
It has been shown that the hemodynamic effect of carboxy-PTIO is minimal in normal rats [13]. This finding was confirmed in our control dogs. This is in marked contrast to the potent peripheral vasoconstriction by non-selective NOS inhibitors [5,7]. The marked increase in systemic blood pressure brought about by well known NOS inhibitors, such as L-NMMA and L-NNA, is due to the complete inhibition of endothelial cNOS. Since NO generated by endothelial cNOS plays vital roles in maintaining organ blood flow due to its vasodilator and antiplatelet aggregation effects, the complete blockade of endothelial cNOS by non-selective NOS inhibitors during septic shock should lead to a marked decrease in organ blood flow and ischemia.
Administration of non-selective NOS inhibitors in septic shock models has been shown to deteriorate metabolic acidosis [7], reduce liver perfusion and induce liver injury [5,22]. In contrast, a recent study from our laboratory has revealed that in LPS-treated rabbits carboxy-PTIO preserved liver energetics, alleviated hepatocellular acidosis, normalized various hydrophilic metabolites such as lactate and alanine in the liver, and decreased plasma concentrations of lactate and pyruvate [23]. These findings suggest that carboxy-PTIO improves hepatocellular metabolic derangement in endotoxin shock models. In this study carboxy-PTIO prevented LPS-induced metabolic acidosis and hypoxia in a dog model, although lactate and hepatic transaminases were not determined. It seems most likely that the marked improvement in metabolic acidosis and hypoxia in septic shock is due to the maintenance of adequate organ perfusion and oxygen delivery by carboxy-PTIO.
However, a major drawback of carboxy-PTIO for its potential use in septic shock is its inactivation by endogenous reducing substances. For example, ascorbic acid has been shown to reduce carboxy-PTIO to a non-radical N-hydroxy derivative, which can no longer scavenge NO [13]. To overcome such fast reduction of nitronyl-nitroxyl radicals, attempts have been made to incorporate nitronyl nitroxide into unilamellar phosphatidylcholine liposomes [24].
It should be noted that hemoglobin may also be used in septic shock models and is as effective an NO scavenger as carboxy-PTIO. It has recently been shown that administration of cross-linked human hemoglobin in a septic pig model improved MAP, but exacerbated pulmonary hypertension and hypoxia [25]. Furthermore, it has been reported that administration of stroma-free soluble hemoglobin worsened hypoxia and acidosis in a septic dog model [26]. Therefore, the therapeutic potential of hemoglobin as an NO scavenger in patients with sepsis appears to be more limited than that of carboxy-PTIO.
In conclusion, our results show that carboxy-PTIO improves blood pressure, metabolic acidosis, and hypoxia in septic shock dogs through scavenging excess NO induced by LPS. Since such NO scavengers preferentially quench the biological action of excess NO without affecting NOS activity, they may represent a promising approach to the treatment of human septic shock. Further studies are needed to design and develop more potent and long-lived nitronyl nitroxide compounds.
References
- Moncada S, Palmer RMJ, Higgs EA. Nitric oxide: Physiology, pathophysiology, and pharmacology. Pharmacol Rev. 1991;43:109–142. [PubMed] [Google Scholar]
- Nathan C. Nitric oxide as a secretory product of mammalian cells. FASEB J. 1992;6:3051–3064. [PubMed] [Google Scholar]
- Kilbourn RG, Griffith OW. Overproduction of nitric oxide in cytokine-mediated and septic shock. J Natl Cancer Inst. 1992;84:827–831. doi: 10.1093/jnci/84.11.827. [DOI] [PubMed] [Google Scholar]
- Nava E, Palmer RMJ, Moncada S. Inhibition of nitric oxide synthesis in septic shock: how much is beneficial? Lancet. 1991;338:1555–1557. doi: 10.1016/0140-6736(91)92375-c. [DOI] [PubMed] [Google Scholar]
- Wright CE, Rees DD, Moncada S. Protective and pathological roles of nirtic oxide in endotoxin shock. Cardiovasc Res. 1992;26:48–57. doi: 10.1093/cvr/26.1.48. [DOI] [PubMed] [Google Scholar]
- Parrillo JE. Pathogenetic mechanisms of septic shock. N Engl J Med. 1993;328:1471–1477. doi: 10.1056/NEJM199305203282008. [DOI] [PubMed] [Google Scholar]
- Mitaka C, Hirata Y, Ichikawa K, et al. Effects of nitric oxide synthase inhibitor on hemodynamic change and O2 delivery in septic dogs. Am J Physiol. 1995;268:H2017–H2023. doi: 10.1152/ajpheart.1995.268.5.H2017. [DOI] [PubMed] [Google Scholar]
- Wu CC, Chen SJ, Szabó C, Thiemermann C, Vane JR. Aminoguanidine attenuates the delayed circulatory failure and improves survival in rodent models of endotoxic shock. Br J Pharmacol. 1995;114:1666–1672. doi: 10.1111/j.1476-5381.1995.tb14955.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mitaka C, Hirata Y, Ichikawa K, Uchida T, Yokoyama K, Amaha K. Effect of aminoguanidine, a more selective inhibitor for inducible nitric oxide synthase, on cardiovascular changes in endotoxin shock dogs. Appl Cardiopulm Pathophys. 1996;6:145–150. [Google Scholar]
- Szabó C, Southan GJ, Thiemermann C. Beneficial effects and improved survival in rodent models of septic shock with S-methylisothiourea sulfate, a potent and selective inhibitor of inducible nitric oxide synthase. Proc Natl Acad Sci USA. 1994; 91:12472–12476. doi: 10.1073/pnas.91.26.12472. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preiser JC, Lejeune P, Roman A, et al. Methylene blue administration in septic shock: a clinical trial. Crit Care Med. 1995;23:259–264. doi: 10.1097/00003246-199502000-00010. [DOI] [PubMed] [Google Scholar]
- Akaike T, Yoshida M, Miyamoto Y, et al. Antagonistic action of imidazolineoxyl N-oxides against endothelium-derived relaxing factor/NO through a radical reaction. Biochemistry . 1993;32:827–832. doi: 10.1021/bi00054a013. [DOI] [PubMed] [Google Scholar]
- Yoshida M, Akaike T, Wada Y, et al. Therapeutic effects of imidazolineoxyl N-oxide against endotoxin shock through its direct nitric oxide-scavenging activity. Biochem Biophys Res Commun. 1994;202:923–930. doi: 10.1006/bbrc.1994.2018. [DOI] [PubMed] [Google Scholar]
- D'Orio V, Wahlen C, Rodriguez LM, et al. A comparison of Escherichia coli endotoxin single bolus injection with low-dose endotoxin infusion on pulmonary and systemic vascular changes. Circ Shock. 1987;21:207–216. [PubMed] [Google Scholar]
- Szabó C, Mitchell JA, Thiemermann C, Vane JR. Nitric oxide-mediated hyporeactivity to noradrenaline precedes the induction of nitric oxide synthase in endotoxin shock. Br J Pharmacol. 1993;108:786–792. doi: 10.1111/j.1476-5381.1993.tb12879.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Szabó C, Salzman AL, Ischiropoulos H. Peroxynitrite-mediated oxidation of dihydrorhodamine 123 occurs in early stages of endotoxic and hemorrhagic shock and ischemia-reperfusion injury. FEBS Lett. 1995;372:229–232. doi: 10.1016/0014-5793(95)00984-h. [DOI] [PubMed] [Google Scholar]
- Maeda H, Akaike T, Yoshida M, Suga M. Multiple functions of nitric oxide in pathophysiology and microbiology: analysis by a new nitric oxide scavenger. J Leukoc Biol. 1994;56:588–592. doi: 10.1002/jlb.56.5.588. [DOI] [PubMed] [Google Scholar]
- Petros A, Bennett D, Vallance P. Effect of nitric oxide synthase inhibitors on hypotension in patients with septic shock. Lancet. 1991;338:1557–1558. doi: 10.1016/0140-6736(91)92376-d. [DOI] [PubMed] [Google Scholar]
- Petros A, Lamb G, Leone A, Moncada S, Bennett D, Vallance P. Effects of a nitric oxide synthase inhibitor in humans with septic shock. Cardiovasc Res. 1994;28:34–39. doi: 10.1093/cvr/28.1.34. [DOI] [PubMed] [Google Scholar]
- Amrani M, OiShea J, Allen NJ, et al. Role of basal release of nitric oxide on coronary flow and mechanical performance of the isolated rat heart. J Physiol. 1992;456:681–687. doi: 10.1113/jphysiol.1992.sp019361. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tsunoda R, Okumura K, Ishizaka H, et al. Vasodilator effect of carboxy-2-phenyl-4,4,5,5-tetramethylimidazoline-1-oxylin the coronary circulation: in vivo and in vitro studies. Eur J Pharmacol. 1994;262:55–63. doi: 10.1016/0014-2999(94)90028-0. [DOI] [PubMed] [Google Scholar]
- Pastor CM, Payen DM. Effect of modifying nitric oxide pathway on liver circulation in a rabbit endotoxin shock model. Shock. 1994;2:196–202. doi: 10.1097/00024382-199409000-00007. [DOI] [PubMed] [Google Scholar]
- Kaneda K, Yoshioka Y, Makika K, Toyooka H, Amaha K. Effect of carboxy-PTIO on systemic hemodynamic, liver energetics and concentration of liver metabolites during endotoxic shock in rabbits: a 31P-and 1H-magnetic resonance spectroscopic study. Crit Care Med. 1997;25:1019–1029. doi: 10.1097/00003246-199706000-00020. [DOI] [PubMed] [Google Scholar]
- Woldman YYu, Khramtsov VV, Grigoríev IA, Kiriljuk IA, Utepbergeno DL. Spin trapping of nitric oxide by nitronyl nitroxides: measurement of the activity of NO synthase from rat cerebellum. Biochem Biophys Res Commun. 1994;202:195–203. doi: 10.1006/bbrc.1994.1912. [DOI] [PubMed] [Google Scholar]
- Aranow JS, Wang H, Zhuang J, Fink MP. Effect of human hemoglobin on systemic and regional hemodynamics in a porcine model of endotoxemic shock. Crit Care Med. 1996;24:807–817. doi: 10.1097/00003246-199605000-00014. [DOI] [PubMed] [Google Scholar]
- Crowley JP, Metzger J, Gray A, Pivacek LE, Cassidy G, Valeri R. Infusion of stroma-free cross-linked hemoglobin during acute gram negative bacteremia. Cric Shock. 1993;41:144–149. [PubMed] [Google Scholar]