
Figure 1.
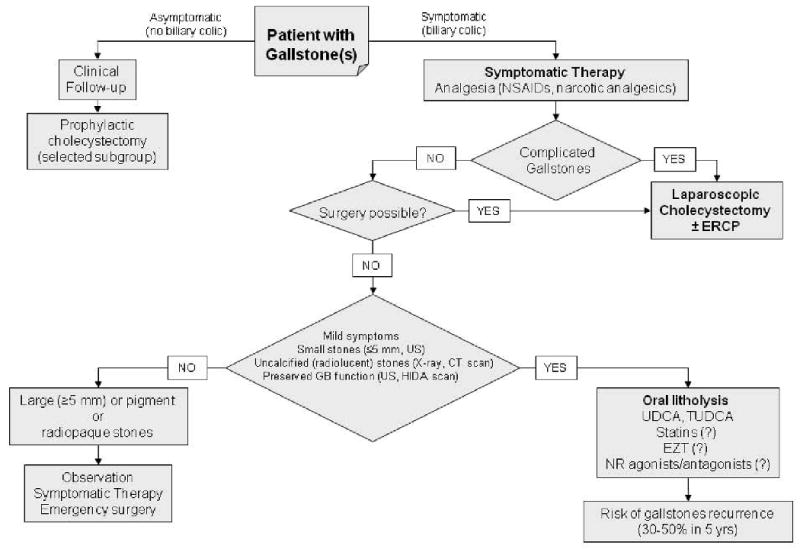
Current therapies of gallstone disease, including cholesterol gallstones (adapted from P. Portincasa et al. (1;36;123)). Novel and potentially effective medical therapies are denoted by the symbol (?). See text for details. Results from meta-analyses indicate surgery as the gold standard for the treating symptomatic gallstones (164-166). Laparoscopic cholecystectomy and small incision cholecystectomy (166), are safe and have similar mortality rate (from 0.1% to 0.7%) (122;165). Both approaches are cost-effective, if compared with open cholecystectomy (165). Compared with open cholecystectomy, both convalescence and hospital stay are shorter and total cost is lower for laparoscopic cholecystectomy (122). Complication rates (including bile duct injuries) are similar between laparoscopic and open cholecystectomy (122;165). When looking at surgical options, a “prophylactic” cholecystectomy can be taken into account in a subgroup of asymptomatic patients bearing a high risk of becoming symptomatic: children (who are exposed to long-term physical presence of stones (167)), morbid obese patients undergoing bariatric surgery (who are at high risk to became symptomatic during rapid weight loss (168)), patients at increased risk for gallbladder cancer (169) (i.e. those with large gallstones, greater than 3 cm) (170;171), a “porcelain” gallbladder (172) or gallbladder polyps rapidly growing or larger than 1 cm). Prophylactic cholecystectomy should also be considered in Native Americans with gallstones, who are at increased risk of gallbladder cancer (3 to 5 percent) (173), and asymptomatic gallstone patients with sickle cell anemia, who form calcium bilirubinate gallstones due to chronic hemolysis and may become symptomatic with recurrent episodes of abdominal pain (174). Prophylactic cholecystectomy has also been proposed in patients with small gallstones and gallbladder dysmotility, since the coexistence of these conditions increases the risk of pancreatitis (51). Abbreviations: CT, computerized tomography; ERCP, endoscopic retrograde cholangiopancreatography; EZT, ezetimibe; HIDA, 99mTc-N-(2,6-dimethylacetanilide)-iminodiacetic acid; GB, gallbladder; GS, gallstones; NR, nuclear receptors; NSAIDs, non-steroidal anti-inflammatory drugs; TUDCA, tauroursodeoxycholic acid; UDCA, ursodeoxycholic acid; US, abdominal ultrasonography.