
Figure 7. Astrocytes mediate functional hyperemia through mGluR5 and glutamate uptake.
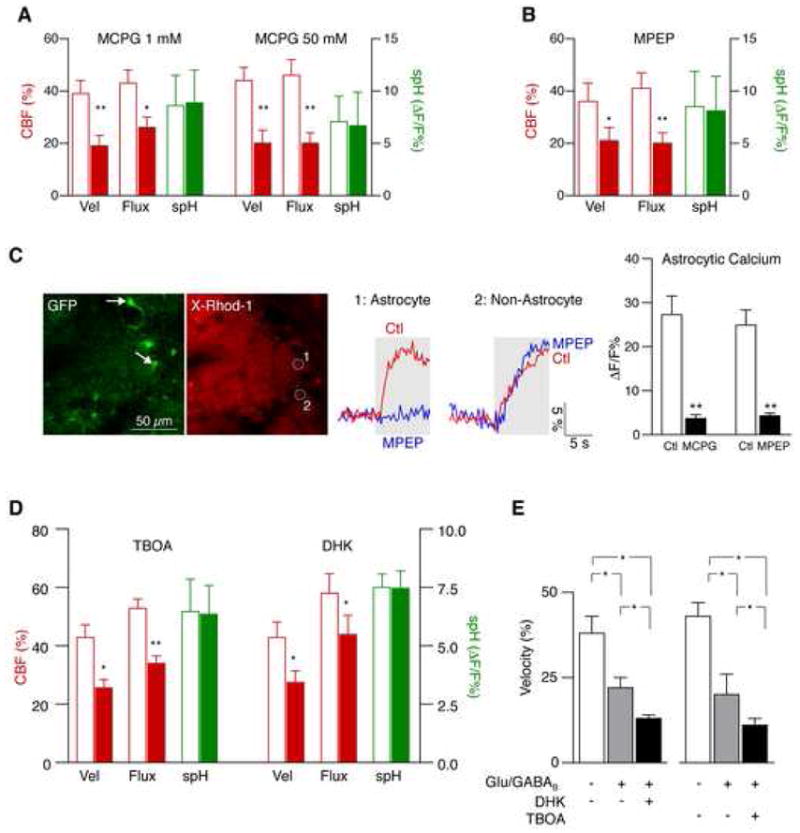
(A–B) Functional hyperemia is mediated in part by astrocytic mGluR5. The broad-spectrum mGluR inhibitor MCPG reduced functional hyperemia at different concentrations (A). The mGluR5 inhibitor MPEP attenuated functional hyperemia to a similar extent (B). Both drugs were applied by local microinjection into the glomerular layer. CBF parameters are relative to baseline. spH responses remained unchanged (mean ± s.e.m.; **p < 0.001, *p < 0.05, paired t-test).
(C) Local mGluR inhibition blocks odor-evoked astrocytic calcium responses. Juxtaglomerular cells (and presynaptic fibers) in GFAP-GFP mice were labeled with X-Rhod-1 AM (red). Astrocytes were identified by their expression of GFP (green, arrows). MCPG and MPEP both blocked calcium responses in astrocytes. MCPG reduced calcium in different cell types, whereas the effect of MPEP was specific for astrocytes, consistent with exclusive expression of mGluR5 in astrocytes in the glomerular layer (mean ± s.e.m., **p < 0.001, paired t-test). Areas 1 and 2 represent calcium signals from an astrocyte (identified by GFP expression) and a GFP-negative cell, respectively. Gray areas represent the duration of odor stimulation.
(D) Astrocytic glutamate uptake also contributes to functional hyperemia. Changes of spH and velocity/flux before and after application of the broad-spectrum glutamate transporter inhibitor TBOA, and dihydrokainate (DHK), a specific blocker of the astrocytic glutamate transporter GLT-1 (mean ± s.e.m.; **p < 0.001, *p < 0.05, paired t-test).
(E) Glutamate transport contributes to functional hyperemia independently from glutamatergic and GABAB receptors. Local inhibition of NMDA, AMPA, mGluR and GABAB receptors reduced functional hyperemia. An additional reduction was observed after blockade of glutamate transporters with TBOA, or by inhibition of astrocytic GLT-1 with DHK (mean ± s.e.m.; *p < 0.05, Repeated Measures ANOVA followed by Tukey Test).