

Abstract
OBJECTIVES
To describe lengths of stay among nursing home decedents.
DESIGN
Retrospective cohort study.
SETTING
The Health and Retirement Study (HRS), a nationally representative survey of U.S. adults aged 50 and older.
PARTICIPANTS
1,817 nursing home residents who died between 1992 and 2006.
MEASUREMENTS
Our primary outcome was length of stay, defined as the number of months between the nursing home admission and the date of death. Covariates included demographic, social, and clinical factors drawn from the HRS interview conducted closest to the date of nursing home admission.
RESULTS
The mean age of decedents was 83.3 (SD 9.0) and the majority were female (59.12%), and White (81.5%). Median and mean length of stay prior to death were 5 months (IQR 1-20) and 13.7 months (SD 18.4), respectively. Fifty-three percent died within 6 months of placement. Large differences in median length of stay were observed by gender (men, 3 months vs. women, 8 months) and net worth (highest quartile, 3 months vs. lowest quartile, 9 months) (all p<.001). These differences persisted after adjustment for age, sex, marital status, net worth, geographic region, and diagnosed chronic conditions (cancer, hypertension, diabetes, lung disease, heart disease, and stroke).
CONCLUSION
Nursing home lengths of stay are brief for the majority of decedents. Lengths of stay varied markedly by factors related to social support.
Keywords: Nursing Home, End of Life, Length of Stay, Palliative Care, Advance Care Planning
INTRODUCTION
Death has become institutionalized over the last 100 years.1 Today, 25% of all deaths in the nation occur in nursing homes and the proportion of all deaths that occur in these settings continues to rise.2 By the year 2020, an estimated 40% of Americans will die in a nursing home.3
While the proportion of overall deaths located in nursing homes has been well described, lengths of stay in nursing homes at the end of life have received little attention. The duration of time residents spend in a nursing home prior to death has important clinical and policy implications. If nursing home lengths of stay tend to be long, then systems and policy directives may improve overall care by prioritizing maintenance and improvement of functional status. If lengths of stay are generally brief at the end of life, then policy ensuring nursing home residents’ access to quality palliative and end-of-life care must be systematized.
We used the Health and Retirement Study (HRS), a nationally representative cohort of older adults, to describe lengths of stay among older adult decedents who resided in nursing homes at the end of life.
MATERIALS AND METHODS
Study Population
We examined a consecutive sample of HRS subjects who died between 1992 and 2006. HRS subjects are a representative sample of Americans over the age of 50 who were living in the community at the time of their initial interview. The HRS is conducted by the Institute for Social Research at the University of Michigan and is sponsored by the National Institute on Aging. The HRS is designed to study transitions in health and wealth among older adults. More information about HRS sampling, data collection procedures and measures can be found on the HRS website (www.hrsonline.isr.umich.edu/).
Subjects were interviewed every two years between 1992 and 2006. Following their death, exit interviews were conducted with family caregivers. Decedents’ primary residence at the end of life was obtained from exit interviews with family caregivers. A nursing home was defined as a facility that provides the following services: dispensing of medication, 24-hour nursing assistance and supervision, personal assistance, and room & meals. A separate question asked about the location of death (nursing home, hospital, home, hospice, or elsewhere), and interviewers were instructed to clarify that residence in a nursing home at the end of life may be distinct from the location of death. Time between the exit interview with the family caregiver and the death of the subject ranged from zero months (i.e., the interview took place during the same month that the subject died) to 59 months. The mean time was one year and 93.4% of family caregivers were interviewed within two years of the subject’s death.
Two thousand three hundred and one subjects primarily resided in a nursing home at the end of life. We excluded subjects with missing information regarding their exact year of placement in nursing home (n=68), age at time of placement in nursing home (n=27), not having completed a core interview within two years of their placement in nursing home (n=203), not having the exact date of death (n=71), having reported nursing home placement after the date of death (n=54) and having an irreconcilable nursing home admission date (i.e. subjects reported as being interviewed in the community after the nursing home admission date) (n=67). Our final sample was comprised of 1,817 decedents. We performed sensitivity analysis to determine how the excluded subjects differ from the subjects in the final sample with regards to demographic characteristics and length of stay in nursing home before death.
Primary Outcome: Length of Stay
In exit interviews, decedents’ caregivers were asked to identify the month and year decedents relocated to the nursing home. The HRS gathers month and year of decedents’ death through proxy interviews and National Death Index records. We used the date of admission to the nursing home and the date of death to calculate length of stay in months. Lengths of stay were considered brief if they were less than 6 months, the prognostic requirement for the Medicare hospice benefit.
Potential Predictors
In the absence of previous studies identifying variables related to lengths of stay in nursing homes at the end of life, we looked at existing literature to identify factors associated with nursing home admission for older adults.2-8 Of those, we selected variables that were available for examination in HRS in order to identify variables that may influence nursing home lengths of stay. Demographic variables include the age at which decedents moved to a nursing home (categorized as <84 and 85 or older in bivariate analysis), sex, and race/ethnicity (categorized as Non-Hispanic White, Non-Hispanic Black, Hispanic, and Non-Hispanic Other.) Data on social and clinical factors are drawn from the last HRS interview before decedents entered a nursing home. The social factors are respondents’ marital status (categorized as Married/Partnered, Not Married/Partnered) and participants’ household net worth (in quartiles). Respondents were asked if they had any of the following diagnosed chronic conditions at the time of nursing home admission: hypertension, diabetes, heart disease, stroke, cancer (except skin cancer), or chronic lung disease (except asthma). Geographical region in which decedents died are drawn from exit interviews with caregivers (categorized as Northeast, Midwest, Southeast, and West).
Analyses
We described lengths of stay in nursing homes at the end of life using a plot of the data and descriptive statistics. Length of stay data had a skewed distribution and, therefore, median length of stay represents the best clinical summary. We performed bivariate analysis using non-parametric methods (Wilcoxon Rank test and Kruskal Wallis test, as appropriate). Multivariate linear regression analysis was used to examine the adjusted associations of demographic, social and clinical factors in relation to lengths of stay in a nursing home at the end of life. Age at time of admission to nursing home, chronic conditions and any other factors significant at a p<.05 level in bivariate analysis were included in the multivariable model. Since the sample size is large, the results of the multiple linear regression are valid even though the normality assumption was not met.9 Additionally, we computed bootstrap estimates of the regression coefficients and their distributions. All statistical analyses were performed using Stata/MP 10.1 and SAS 9.1.3. The institutional review board at the University of California, San Francisco considered this study exempt.
RESULTS
Study population
Over the years 1992 to 2006, 8,433 HRS participants died, and 27.3% of these decedents resided in a nursing home at the time of death. While subjects resided in a nursing home at the end of life, their physical location of death was distinct for many. Of the 1,817 subjects in our study sample who resided in a nursing home at the end of life, next-of-kin stated that the physical location of death was the nursing home for 70.4% of subjects, the hospital for 22.6%, in-inpatient hospice facilities for 3.5%, home for 0.4%, and 3.1% died elsewhere. The majority of decedents were Non-Hispanic White (81.5%), female (59.1%), and had a mean age of 83.3 (SD 9.0) years at the time of admission to a nursing home (Table 1).
Table 1.
Characteristics of study sample (N=1,817)
| Characteristic | Percent* | |
|---|---|---|
| Demographics | Age at Placement, mean (SD) | 83.3 (9.0) |
| Age at Placement 85 or older | 50.6 | |
| Male, % | 40.9 | |
| Race / Ethnicity, % | ||
| Non-Hispanic White | 81.5 | |
| Non-Hispanic Black | 14.0 | |
| Hispanic | 2.9 | |
| Other | 1.6 | |
| Marital Status at Placement, % | ||
| Married/Partnered | 36.1 | |
| Social Factors | SES | |
| Household net worth, median (IQR) | $50,000 ($3000-$150,000) | |
| Region Died, % | ||
| Midwest | 32.4 | |
| South | 28.8 | |
| Northeast | 24.7 | |
| West | 14.1 | |
| Chronic Diseases | ||
| Cancer, % | 17.4 | |
| Hypertension, % | 58.2 | |
| Diabetes, % | 22.8 | |
| Lung Disease, % | 14.8 | |
| Heart Disease, % | 44.6 | |
| Stroke, % | 24.8 | |
| Number of Chronic Disease, % | ||
| 0 | 14.9 | |
| 1 | 28.5 | |
| 2 | 28.0 | |
| 3 | 18.9 | |
| 4 or more | 9.7 |
The values in this column represent the percent of the sample in the given subgroup, except for the age and household net worth variables.
Analysis of the 484 subjects excluded from our analysis due to missing data revealed that those subjects were similar to the subjects included in the sample in age at the time of placement in nursing home, household net worth and length of stay in nursing home before death. They were, however, more likely to be female (64.3% vs. 59.1%, p=0.040) and Hispanic (5.6% vs. 2.9%, p=0.004).
Length of stay in nursing homes at the end of life
Decedents’ lengths of stay in nursing homes at the end of life are illustrated in the Figure. The mean length of stay among decedents was 13.7 months; however, this was explained by a relatively small number of subjects with long lengths of stay. The median length of stay was only 5 months (IQR 1-20). The majority of residents had short lengths of stay, 65% percent of decedents had lengths of stay of less than one year, and over 53% died within 6 months of admission.
Bivariate analysis identified statistically significant associations between lengths of stay and gender, marital status, household net worth, region of death, all chronic conditions but hypertension, and the number of chronic conditions (Table 2). Men spent fewer months (median of 3 months) in a long-term care setting prior to death than women (median of 8 months) (p<.0001). Those who were married at the time of placement had median lengths of stay 4 months shorter than those who were unmarried (p<.0001). Decedents in the highest quartile of net worth (household net worth > $150,000) had median lengths of stay 6 months shorter than the median stays of the lowest quartile (household net worth < $3,000) (p <.0001). There was regional variation in average length of stay; decedents in the West had median nursing home lengths of stays that were 2 months shorter than decedents in the Midwest and 3 months shorter than decedents in the South or Northeast (p=0.015). Having a chronic illness was associated with statistically significant differences in lengths of stay. Lengths of stay were shortest for patients suffering from cancer or lung disease (median of 3 months). There were no statistically significant associations between lengths of stay and decedents’ race or ethnicity.
Table 2.
Factors associated with length of stay among residents who resided in a nursing home near death: bivariate analysis
| Factor | Mean (SD) LOS in Months | Minimum – Maximum LOS in Months | Median (25th percentile - 75th percentile) LOS in Months | P-value* |
|---|---|---|---|---|
| Total Sample | 13.7 (18.4) | 0-121 | 5 (1-20) | |
| Age at Placement | ||||
| ≤ 84 | 14.0 (20.2) | 0-121 | 5 (1-20) | 0.067 |
| ≥ 85 | 13.4 (16.5) | 0-82 | 6 (1-20) | |
| Women | 16.0 (19.3) | 0-121 | 8 (2-24) | <0.0001 |
| Men | 10.3 (16.5) | 0-105 | 3 (1-13) | |
| Race / Ethnicity | ||||
| Non-Hispanic White | 13.2 (17.6) | 0-121 | 5 (1-20) | |
| Non-Hispanic Black | 16.4 (22.1) | 0-118 | 6.5 (2-23) | 0.098 |
| Hispanic | 16.2 (21.9) | 0-105 | 6 (1.5-24) | |
| Other | 8.4 (10.7) | 0-34 | 2 (1-21) | |
| Marital Status | ||||
| Not Married | 14.7 (18.4) | 0-121 | 7 (2-22) | <0.0001 |
| Married/Partnered | 11.8 (18.2) | 0-105 | 3 (1-16.5) | |
| Household Net Worth | ||||
| Quartile 1 (lowest) | 17.0 (19.8) | 0-106 | 9 (2-25) | <0.0001 |
| Quartile 2 | 14.8 (20.1) | 0-121 | 6 (1-22) | |
| Quartile 3 | 12.3 (17.2) | 0-88 | 5 (1-17) | |
| Quartile 4 | 10.4 (15.4) | 0-100 | 3 (1-14) | |
| Region of Death | ||||
| Midwest | 13.7 (18.5) | 0-121 | 5 (1-21) | |
| South | 14.6 (19.5) | 0-118 | 6 (1-22) | 0.015 |
| Northeast | 14.0 (17.7) | 0-84 | 6 (1-22) | |
| West | 11.0 (16.8) | 0-88 | 3 (1-14) | |
| Chronic Conditions | ||||
| Cancer | 9.8 (15.7) | 0-105 | 3 (1-12) | <0.001 |
| No Cancer | 14.5 (18.8) | 0-121 | 6 (1-21.5) | |
| Hypertension | 12.9 (17.2) | 0-118 | 5 (1-19) | 0.503 |
| No Hypertension | 14.7 (19.9) | 0-121 | 5 (1-22) | |
| Diabetes | 11.5 (16.2) | 0-118 | 4 (1-17) | 0.018 |
| No Diabetes | 14.2 (18.9) | 0-121 | 6 (1-21) | |
| Lung Disease | 10.1 (16.2) | 0-118 | 3 (1-12.5) | <0.0001 |
| No Lung Disease | 14.2 (18.6) | 0-121 | 6 (1-21) | |
| Heart Disease | 11.5 (15.7) | 0-118 | 5 (1-17) | 0.005 |
| No Heart Disease | 15.4 (20.2) | 0-121 | 6 (1-23) | |
| Stroke | 15.4 (19.9) | 0-118 | 7 (2-22) | 0.005 |
| No Stroke | 13.1 (17.8) | 0-121 | 5 (1-19) | |
| Number of Chronic Illnesses | ||||
| 0 | 17.7 (21.8) | 0-121 | 8 (1-28) | 0.001 |
| 1 | 15.6 (19.9) | 0-92 | 6 (1-24) | |
| 2 | 12.1 (16.6) | 0-105 | 5 (1-17) | |
| 3 | 11.3 (15.8) | 0-105 | 4 (1-16) | |
| 4 or more | 10.8 (15.6) | 0-118 | 4 (1-17) | |
Tests for the equality of the medians, performed using Wilcoxon-Man-Whitney test or Kruskal- Wallis test.
Multivariate linear regression analysis revealed that male gender, high household net worth, and diagnoses of cancer, hypertension, diabetes, lung disease, or heart disease were associated with shorter lengths of stay after adjusting for all other potential predictors (Table 3). Residents with a history of stroke had longer lengths of stay than those without a history of stroke. Bootstrap estimates and corresponding p-values were very similar and therefore are not reported here.
Table 3.
Independent factors associated with length of stay among residents who resided in a nursing home near death: multivariate linear regression analysis
| Factor | Beta | Std. Error | P-value |
|---|---|---|---|
| Age at Placement | -0.1 | 0.1 | 0.122 |
| Sex | |||
| Female | Ref | ||
| Male | -5.1 | 0.9 | <0.001 |
| Marital Status | |||
| Not Married | Ref | ||
| Married/Partnered | 0.4 | 1.0 | 0.703 |
| Household Net Worth | |||
| Quartile 1 (lowest) | Ref | ||
| Quartile 2 | -1.1 | 1.2 | 0.375 |
| Quartile 3 | -3.4 | 1.2 | 0.005 |
| Quartile 4 | -5.2 | 1.3 | <0.001 |
| Region of Death | |||
| Midwest | Ref | ||
| South | 0.6 | 1.1 | 0.558 |
| Northeast | -0.7 | 1.1 | 0.548 |
| West | -2.2 | 1.3 | 0.098 |
| Chronic Diseases | |||
| No Cancer | Ref | ||
| Cancer | -3.9 | 1.1 | <0.001 |
| Ho Hypertension | Ref | ||
| Hypertension | -2.6 | 0.9 | 0.004 |
| No Diabetes | Ref | ||
| Diabetes | -2.4 | 1.1 | 0.024 |
| No Lung Disease | Ref | ||
| Lung Disease | -3.1 | 1.2 | 0.010 |
| No Heart Disease | Ref | ||
| Heart Disease | -3.5 | 0.9 | <0.001 |
| No Stroke | Ref | ||
| Stroke | 3.4 | 1.0 | 0.001 |
DISCUSSION
In this sample of 1,817 older adults who were living in nursing homes at the end of life, we found that lengths of stay for the majority of decedents were brief: less than six months. We also found that decedents’ lengths of stay differed according to a number of demographic, social, and clinical factors and some of these differences were dramatic. Demographic and social indicators often related to having increased access to paid and informal caregiver support include being male, married, and having a higher net worth.10 These indicators revealed significantly shorter nursing home lengths of stay at the end of life. Additionally, those who were diagnosed with a chronic illness often associated with rapid functional decline, such as cancer, had shorter median lengths of stay at the end of life than those diagnosed with an illness generally associated with more progressive functional decline, such as stroke or heart disease.
Brief lengths of stay at the end of life coupled with the variability that exists among subgroups highlights the importance of addressing advance care planning needs with residents and families, as there may be shorter periods of time to address important end-of-life tasks with some residents than with others. There is growing support for the notion that advance care planning conversations, including hospice and palliative care options, ought to occur shortly after admission and be readdressed periodically with nursing home residents and their families.11, 12 Currently, many nursing home residents do not have any documentation of advance directives. In 2004 only 44% of nursing home residents had any advance directive recorded at admission and only 63% of residents had any advance directive orders after 12 months in the nursing home.13 Yet, lengths of stay (and life) were within the window of hospice eligibility for most patients among this sample of decedents at the time of nursing home admission.
While the rates of hospice use in our sample are unknown, hospice care appears to be underutilized in long-term care settings.11, 12, 14 Currently, estimates of the proportion of nursing home decedents in the United States who received hospice or palliative care range from less than 10% to 30% 15, 16. Research suggests that hospice care improves the quality of life at the end-of-life in long term care settings. A 2002 study by Miller and colleagues found that 51% of dying nursing home residents who were enrolled in hospice (n=2,644) received analgesics for daily pain, compared to 33% of non-hospice residents (n=7,929)17. Family satisfaction with symptom care has been shown to be superior for long-term care residents enrolled in hospice compared to non-hospice residents.18 Evidence suggests that non-hospice palliative care teams and palliative care education for nursing home staff improves patient care19. Unlike hospice care, which is bound by criteria related to prognosis and goals of care, non-hospice palliative care may be offered in conjunction with curative treatments for chronically or terminally ill residents despite their expected prognosis, code status, or treatment plan. Unfortunately, while many nursing homes have some affiliation with a hospice, few nursing home providers have received any training in palliative care.11, 14, 20
These findings may have important implications for nursing home care, as it now often focuses on rehabilitation.11, 12 A 1991 survey of North Carolina nursing homes reported 8 percent of patients were in daily specialized rehabilitation.21 By 2006, however, rehabilitation accounted for 86 percent of all Medicare reimbursement days in skilled nursing facilities nationwide22. Many of these changes are due to financial policy rather than clinical factors.23 Rehabilitation is an important goal for many, but some patients may benefit more from a palliative approach24-26.
Though over half of decedents resided in a long-term care setting for less than six months before death, the range in lengths of stay within this study population was large (ranging from less than one month to more than 10 years). Eligibility for the Medicare hospice benefit is prognosis based: patients must have a physician estimated prognosis of less than six months to live. While we do not have data in our study on the expected prognosis of subjects at the time of admission, in general, prognosis for nursing home residents can be difficult to determine.27-29 The Medicare hospice benefit may more appropriately and effectively serve older adults at the end of life if eligibility criteria were redefined by symptom and psychosocial needs, rather than prognosis.
Unlike our study, previous studies have been limited to describing nursing home residents whose physical location of death was the nursing home, excluding those who resided in a nursing home near the end of life but were transferred to the hospital in the hours or days prior to death 2, 30-32. For these patients, however, the optimal time and place to address palliative needs is likely the nursing home setting where they spend the last weeks or months of life, not the hospital where they spend the final moments prior to death33.
Limitations of this study are noted. The HRS enrolls community dwelling older adults and tracks them over time as they age and enter nursing homes. Additionally, the few residents of nursing homes admitted at a younger age would not be captured in this study, biasing our findings toward shorter lengths of stay. We relied on after death interviews with next-of-kin to determine the admission date to the nursing home. In addition to the issue of recall bias, lengths of stays for nursing home residents who were transferred to the hospital due to acute illness and then later readmitted may not be accurately presented in this study. However, subjects’ next-of-kin are unlikely to have counted readmission to the nursing home after hospitalization as a new start date. In this way our data may be superior to administrative data that count only the length of stay for the final admission prior to death. We do not know the reason for admission to the nursing home, and some patients may have been admitted specifically for end-of-life care. We excluded patients admitted to residential hospice facilities, although some residential hospice facilities may have been located within nursing homes. Given the complexities of the study design, we were unable to track time trends in nursing home use in the HRS. The prognoses for patients in our study were not known at the time of admission. Retrospective studies of end-of-life care have been criticized as identifying patients who are dying can be challenging for clinicians;34 thus, studies of the dying differ from studies of decedents.35 However, studies of decedents may offer utility in identifying patterns that add incrementally to our understanding of how to care for patients at the end of life.36
Future prospective studies in this area are needed to further examine trends in nursing home lengths of stay at the end of life over time, and identify additional clinical and social indicators that may be significantly associated, such as functional status, expected prognosis at admission, and the number of hospital readmissions that take place prior to death. Authors of this study are in the process of linking HRS data to Medicare claim data to identify those patients who utilize hospice benefits or acute care services at the end of life. Given that median lengths of stay in a nursing home were less than a year, studies are also needed to examine the possible fiscal implications nursing home lengths of may have for individuals interested in purchasing long term care insurance.
In conclusion, brief nursing home lengths of stay among older adult decedents highlight the importance for health care providers to discuss and address advance care planning needs with patients and families, including palliative and hospice care options, soon after admission to the nursing home.
Figure 1.
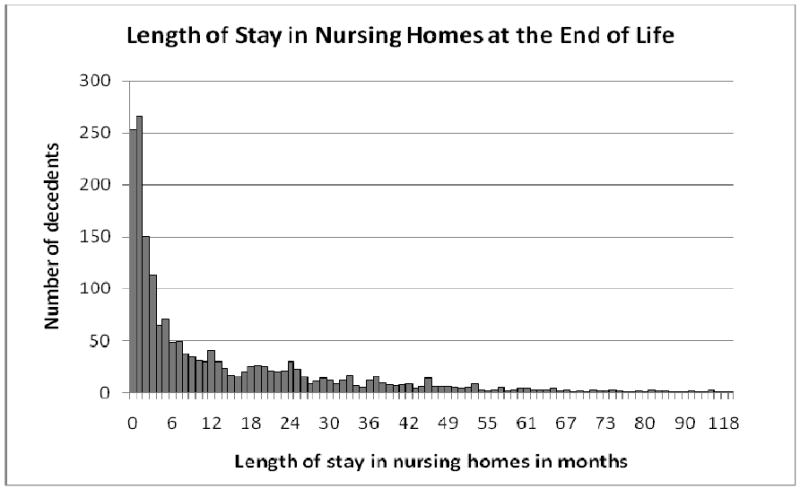
Lengths of stay among subjects who resided in a nursing home at death
Acknowledgments
Funding Sources: Dr. Smith is supported by a Research Supplement to Promote Diversity in Health Related Research from the National Institute on Aging (R01AG028481), the University of California San Francisco Clinical and Translational Science Institute (UL1 RR024131), and the National Palliative Care Research Center.
Sponsor’s Role: The National Institute of Health and the National Palliative Care Research Center had no role in the design, methods, subject recruitment, data collections, analysis, or preparation of the paper.
Footnotes
Author Contributions: All authors were involved in the study concept and design, Drs. Smith and Covinsky were responsible for the acquisition of data, and all authors were involved in the analysis and interpretation of data and preparation of the manuscript.
Conflict of Interest: The editor in chief has reviewed the conflict of interest checklist provided by the authors and has determined that the authors have no financial or any other kind of personal conflicts with this paper.
References
- 1.Katz BP, Zdeb MS, Therriault GD. Where people die. Public Health Rep. 1979;94:522–527. [PMC free article] [PubMed] [Google Scholar]
- 2.Gruneir A, Mor V, Weitzen S, et al. Where people die: A multilevel approach to understanding influences on site of death in America. Med Care Res Rev. 2007;64:351–378. doi: 10.1177/1077558707301810. [DOI] [PubMed] [Google Scholar]
- 3.Weitzen S, Teno JM, Fennell M, et al. Factors associated with site of death: A national study of where people die. Med Care. 2003;41:323–335. doi: 10.1097/01.MLR.0000044913.37084.27. [DOI] [PubMed] [Google Scholar]
- 4.Bharucha AJ, Pandav R, Shen C, et al. Predictors of nursing facility admission: A 12-year epidemiological study in the United States. J Am Geriatr Soc. 2004;52:434–439. doi: 10.1111/j.1532-5415.2004.52118.x. [DOI] [PubMed] [Google Scholar]
- 5.Yaffe K, Fox P, Newcomer R, et al. Patient and caregiver characteristics and nursing home placement in patients with dementia. JAM. 2002;287:2090–2097. doi: 10.1001/jama.287.16.2090. [DOI] [PubMed] [Google Scholar]
- 6.Brock DB, Foley DJ, Salive ME. Hospital and nursing home use in the last three months of life. J Aging Healt. 1996;8:307–319. doi: 10.1177/089826439600800301. [DOI] [PubMed] [Google Scholar]
- 7.Andel R, Hyer K, Slack A. Risk factors for nursing home placement in older adults with and without dementia. J Aging Healt. 2007;19:213–228. doi: 10.1177/0898264307299359. [DOI] [PubMed] [Google Scholar]
- 8.Mitchell SL, Teno JM, Miller SC, et al. A national study of the location of death for older persons with dementia. J Am Geriatr Soc. 2005;53:299–305. doi: 10.1111/j.1532-5415.2005.53118.x. [DOI] [PubMed] [Google Scholar]
- 9.Lumley T, Diehr P, Emerson S, et al. The importance of the normality assumption in large public health data sets. Annu Rev Public Health. 2002;23:151–169. doi: 10.1146/annurev.publhealth.23.100901.140546. [DOI] [PubMed] [Google Scholar]
- 10.Katz SJ, Kabeto M, Langa KM. Gender disparities in the receipt of home care for elderly people with disability in the United States. JAMA. 2000;284:3022–3027. doi: 10.1001/jama.284.23.3022. [DOI] [PubMed] [Google Scholar]
- 11.Meier DE, Lim B, Carlson MD. Raising the standard: palliative care in nursing homes. Health Aff (Millwood) 29:136–140. doi: 10.1377/hlthaff.2009.0912. [DOI] [PubMed] [Google Scholar]
- 12.Hirschman K, Kapo J, Straton JB, et al. Hospice in Long-Term Care. Ann Long-Term Care. 2005;13:25–29. [Google Scholar]
- 13.McAuley WJ, Buchanan RJ, Travis SS, et al. Recent trends in advance directives at nursing home admission and one year after admission. Gerontologist. 2006;46:377–381. doi: 10.1093/geront/46.3.377. [DOI] [PubMed] [Google Scholar]
- 14.Zerzan J, Stearns S, Hanson L. Access to palliative care and hospice in nursing homes. JAMA. 2000;284:2489–2494. doi: 10.1001/jama.284.19.2489. [DOI] [PubMed] [Google Scholar]
- 15.Bercovitz A, Decker FH, Jones A, et al. End-of-life care in nursing homes: 2004 National Nursing Home Survey. Natl Health Stat Report. 2008:1–23. [PubMed] [Google Scholar]
- 16.Miller SC, Han B. End-of-life care in U.S. nursing homes: Nursing homes with special programs and trained staff for hospice or palliative/end-of-life care. J Palliat Med. 2008;11:866–877. doi: 10.1089/jpm.2007.0278. [DOI] [PubMed] [Google Scholar]
- 17.Miller SC, Mor V, Wu N, et al. Does receipt of hospice care in nursing homes improve the management of pain at the end of life? J Am Geriatr Soc. 2002;50:507–515. doi: 10.1046/j.1532-5415.2002.50118.x. [DOI] [PubMed] [Google Scholar]
- 18.Baer WM, Hanson LC. Families’ perception of the added value of hospice in the nursing home. J Am Geriatr Soc. 2000;48:879–882. doi: 10.1111/j.1532-5415.2000.tb06883.x. [DOI] [PubMed] [Google Scholar]
- 19.Hanson LC, Reynolds KS, Henderson M, et al. A quality improvement intervention to increase palliative care in nursing homes. J Palliat Med. 2005;8:576–584. doi: 10.1089/jpm.2005.8.576. [DOI] [PubMed] [Google Scholar]
- 20.Chang A, Walter L. Recognizing dementia is a terminal illness in nursing home residents. Arch Intern Med. doi: 10.1001/archinternmed.2010.166. In Press. [DOI] [PubMed] [Google Scholar]
- 21.Kochersberger G, Hielema F, Westlund R. Rehabilitation in the nursing home: How much, why, and with what results. Public Health Rep. 1994;109:372–376. [PMC free article] [PubMed] [Google Scholar]
- 22.MEDPAC. A Data Book: Healthcare spending and the Medicare program. Commission MPA, ed 2008 June; [Google Scholar]
- 23.Buntin MB. Access to postacute rehabilitation. Arch Phys Med Rehabil. 2007;88:1488–1493. doi: 10.1016/j.apmr.2007.07.023. [DOI] [PubMed] [Google Scholar]
- 24.Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56:2171–2179. doi: 10.1111/j.1532-5415.2008.02023.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Kurella Tamura M, Covinsky KE, Chertow GM, et al. Functional Status of Elderly Adults before and after Initiation of Dialysis. N Engl J Med. 2009;361:1539–1547. doi: 10.1056/NEJMoa0904655. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Arnold RM, Zeidel ML. Dialysis in frail elders--a role for palliative care. N Engl J Med. 2009;361:1597–1598. doi: 10.1056/NEJMe0907698. [DOI] [PubMed] [Google Scholar]
- 27.Murray SA, Kendall M, Boyd K, et al. Illness trajectories and palliative care. BMJ. 2005;330:1007–1011. doi: 10.1136/bmj.330.7498.1007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Flacker JM, Kiely DK. Mortality-related factors and 1-year survival in nursing home residents. J Am Geriatr Soc. 2003;51:213–221. doi: 10.1046/j.1532-5415.2003.51060.x. [DOI] [PubMed] [Google Scholar]
- 29.Mitchell SL, Teno JM, Kiely DK, et al. The clinical course of advanced dementia. N Engl J Med. 2009;361:1529–1538. doi: 10.1056/NEJMoa0902234. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Hanson LC, Eckert JK, Dobbs D, et al. Symptom experience of dying long-term care residents. J Am Geriatr Soc. 2008;56:91–98. doi: 10.1111/j.1532-5415.2007.01388.x. [DOI] [PubMed] [Google Scholar]
- 31.Teno JM, Clarridge BR, Casey V, et al. Family perspectives on end-of-life care at the last place of care. JAMA. 2004;291:88–93. doi: 10.1001/jama.291.1.88. [DOI] [PubMed] [Google Scholar]
- 32.Miller SC, Gozalo P, Mor V. Hospice enrollment and hospitalization of dying nursing home patients. Am J Med. 2001;111:38–44. doi: 10.1016/s0002-9343(01)00747-1. [DOI] [PubMed] [Google Scholar]
- 33.Miller SC, Teno JM, Mor V. Hospice and palliative care in nursing homes. Clin Geriatr Med. 2004;20:717–734. vii. doi: 10.1016/j.cger.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 34.Christakis NA, Lamont EB. Extent and determinants of error in doctors’ prognoses in terminally ill patients: Prospective cohort study. BMJ. 2000;320:469–472. doi: 10.1136/bmj.320.7233.469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Bach PB, Schrag D, Begg CB. Resurrecting treatment histories of dead patients: A study design that should be laid to rest. JAMA. 2004;292:2765–2770. doi: 10.1001/jama.292.22.2765. [DOI] [PubMed] [Google Scholar]
- 36.Earle CC, Ayanian JZ. Looking back from death: The value of retrospective studies of end-of-life care. J Clin Oncol. 2006;24:838–840. doi: 10.1200/JCO.2005.03.9388. [DOI] [PubMed] [Google Scholar]