
Figure 1.
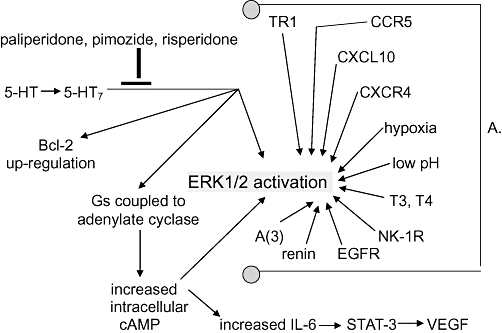
A schema drawn from data presented in text. Some of these relationships are putative, empirically demonstrated not causally established. For example it has not been shown that Bcl-2 up-regulation after 5-HT7 ligation of serotonin is not secondary to adenylate cyclase activation, or to STAT-3 activation, or to ERK1/2 activation, or to none of these, or to some combination of these. Which of the three suggested drugs is best at 5-HT7 signalling inhibition is unknown. Note the crowd of arrows pointing to ERK1/2 activation (phosphorylation). That's a problem. In all likelihood they can to at least some degree cross-cover for each other so that each of these and more must be inhibited for cure. A. Some routes to ERK1/2 in glioblastoma. CCR5 is the chemokine receptor (synonomous with CD195) for RANTES (regulated upon activation, normal T-cell expressed and secreted, synonomous with CCL5). CXCL10 is the 10 kDa ligand for CXCR3. CXCR4 is the receptor for CXCL12. T3 is liothyronine, and T4 is levothyroxine. NK-1R is the receptor for the 11-amino-acid peptide neurotransmitter substance P. EGFR is epidermal growth factor receptor (synonomous with HER-1). A(3) is the adenosine receptor 3. TR1 is the transferring receptor 1. 5-HT, serotonin; 5-HT7, the serotonin receptor 7; cAMP, cyclic ademosine monophosphate; ERK1/2, extracellular regulated kinase 1/2; IL-6, interleukin-6; STAT-3, signal transducer and activator of transcription-3; VEGF, vascular endothelial growth factor.