
Fig. 1.
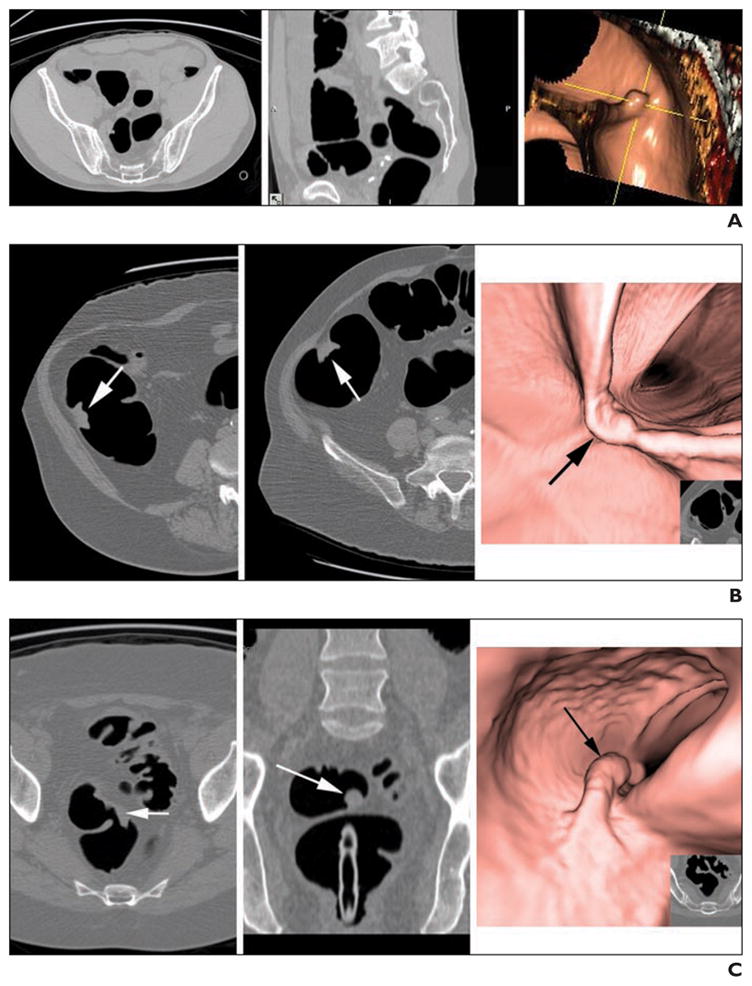
Examples of easy-to-detect, moderate-to-detect, and difficult-to-detect polyps used at qualification testing.
A, CT colonography (CTC) example of easy-to-detect polyp in 58-year-old man. Axial (left), sagittal (middle), and 3D (right) views are shown. Imaging was performed with patient in prone position. Rectosigmoid colon was collapsed while patient was in supine position. This 8-mm tubular adenoma was detected by all radiologists.
B, CTC example of moderate-to-detect cancer (arrows) in 52-year-old man with proximal occlusive sigmoid cancer. Cancer is shown on axial prone (left) and supine (middle and right) CTC images. This ascending colon cancer growing along fold was missed at initial endoscopic assessment but was confirmed at surgery. At initial qualification testing, 80% (12/15) of radiologists identified this lesion.
C, CTC example of difficult-to-detect rectal polyp (arrows) in 50-year-old woman. Prone axial (left), prone coronal (middle), and 3D (right) views are shown. This polyp was detected by only 20% (3/15) of radiologists at qualification testing. Polyp was difficult to detect because only portion of lesion can be seen in any one view, with stalk lying along inferior rectal wall on prone images. Rectosigmoid was collapsed in supine view. Pathology showed 2.5-cm pedunculated tubular adenoma.