

Abstract
An 8-year old boy with a small goiter, normal basal metabolic rate (BMR), and elevated serum thyroid hormone levels (thyroxine [T4] 19.5 μg per 100 ml, free T4 4 ng per 100 ml, triiodothyronine [T3] 505 ng per 100 ml) was studied. He had measurable serum thyroid-stimulating hormone (TSH) levels (average 5.5 μU per ml), and the thyroxine-binding proteins, hearing, and epiphyseal structures were normal. There was no parental consanguinity nor were there thyroid abnormalities either in the parents or six siblings.
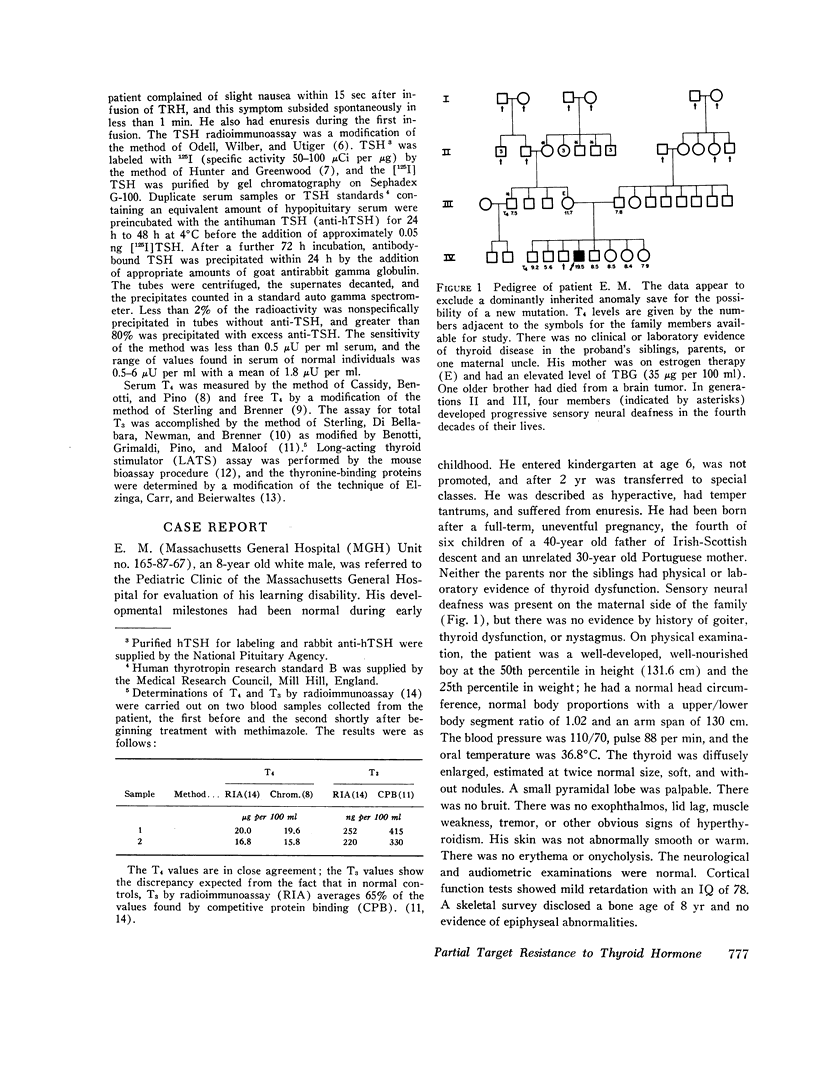
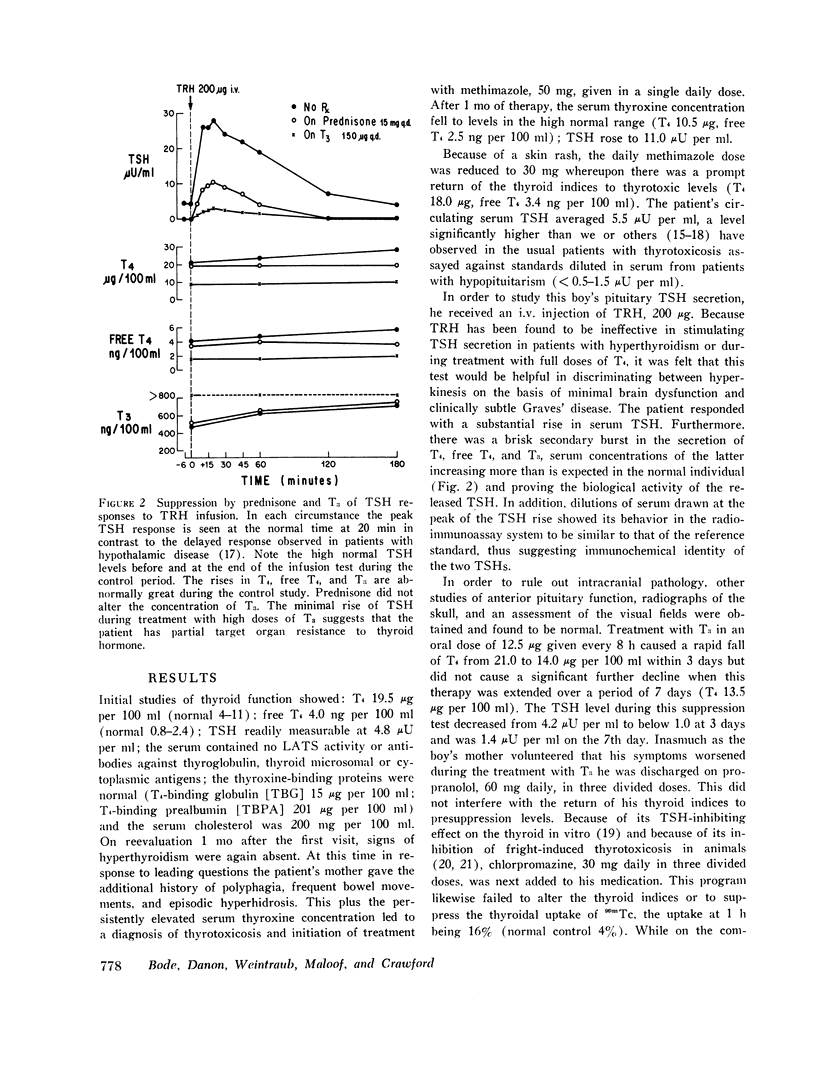
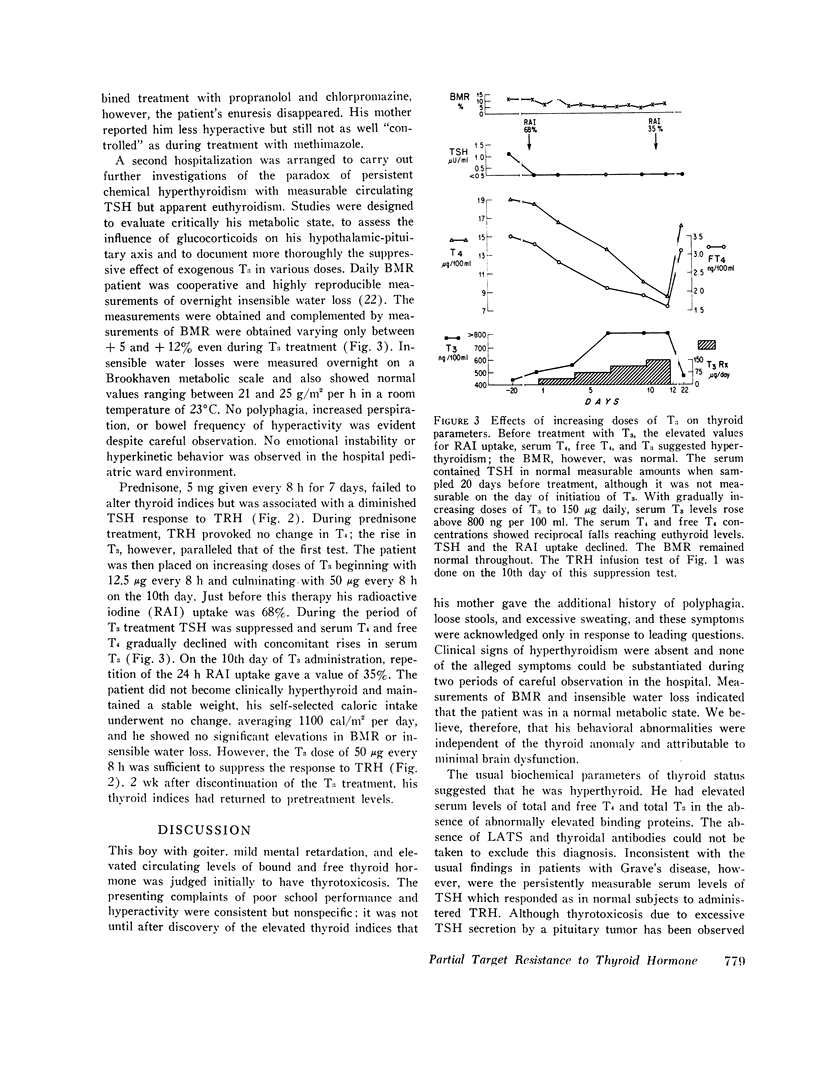
Methimazole, 50 mg daily, depressed thyroxine synthesis (T4 10.5, free T4 2.5) and caused a rise in TSH to 11 μU per ml. After discontinuation of treatment, TSH declined to 4.2 μU per ml and chemical hyperthyroidism returned (T4 21.0 μg per 100 ml, free T4 4.2, and total T3 475 ng per 100 ml, radioactive iodine [RAI] uptake 68%), but studies of BMR and insensible water loss showed the patient to be clinically euthyroid. Thyrotropin-releasing hormone (TRH), 200 μg i.v., caused a brisk rise in TSH to 28 μU per ml, with T4 rising to 28 μg per 100 ml, free T4 to 5.6, and T3 to 730 ng per 100 ml, thus indicating that the pituitary-thyroid system was intact and that the patient's TSH was biologically active. The unusual sensitivity of the pituitary cells to TRH in spite of the markedly elevated serum thyroid hormone levels also suggested that the pituitary was insensitive to suppression by T3 or T4. Serum dilution studies gave immunochemical evidence that this patient's TSH was normal. Neither propranolol, 60 mg, chlorpromazine, 30 mg, nor prednisone, 15 mg daily, influenced thyroid indices. Steroid treatment, however, suppressed the pituitary response to TRH, T3 in doses increased over a period of 12 days to as much as 150 μg daily caused a rise in serum T3 to above 800 ng per 100 ml, a decline of T4 to euthyroid levels (T4 9.5 μg per 100 ml, free T4 1.6 ng per 100 ml), suppression of the RAI uptake from 68% to 35%, and marked blunting of the responses to TRH, but the BMR and insensible water loss remained normal. The data suggest that the patient's disorder is due to partial resistance to thyroid hormone.
Full text
PDF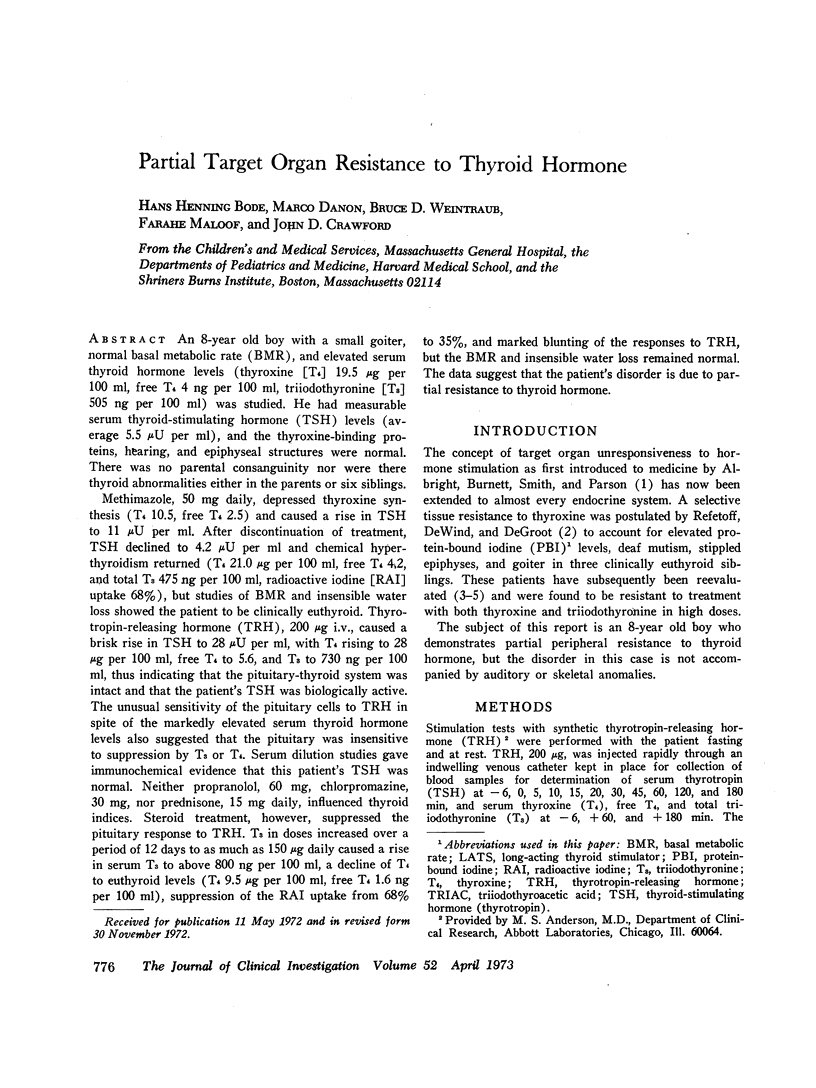
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cassidy C. E., Benotti J., Peno S. Clinical evaluation of the determination of thyroxine iodine. J Clin Endocrinol Metab. 1968 Mar;28(3):420–421. doi: 10.1210/jcem-28-3-420. [DOI] [PubMed] [Google Scholar]
- ELZINGA K. E., CARR E. A., Jr, BEIERWALTES W. H. Adaptation of the standard Durrum-type cell for reverse-flow paper electrophoresis. Am J Clin Pathol. 1961 Aug;36:125–131. doi: 10.1093/ajcp/36.2.125. [DOI] [PubMed] [Google Scholar]
- Emerson C. H., Utiger R. D. Hyperthyroidism and excessive thyrotropin secretion. N Engl J Med. 1972 Aug 17;287(7):328–333. doi: 10.1056/NEJM197208172870704. [DOI] [PubMed] [Google Scholar]
- Fleischer N., Burgus R., Vale W., Dunn T., Guillemin R. Preliminary observations on the effect of synthetic thyrotropin releasing factor on plasma thyrotropin levels in man. J Clin Endocrinol Metab. 1970 Jul;31(1):109–112. doi: 10.1210/jcem-31-1-109. [DOI] [PubMed] [Google Scholar]
- Galton V. A., Inggar S. H., Jimenez-Fonseca J., Hershman J. M. Alterations in thyroid hormone economy in patients with hydatidiform mole. J Clin Invest. 1971 Jun;50(6):1345–1354. doi: 10.1172/JCI106614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- HUNTER W. M., GREENWOOD F. C. Preparation of iodine-131 labelled human growth hormone of high specific activity. Nature. 1962 May 5;194:495–496. doi: 10.1038/194495a0. [DOI] [PubMed] [Google Scholar]
- Hershman J. M., Pittman J. A., Jr Utility of the radioimmunoassay of serum thyrotrophin in man. Ann Intern Med. 1971 Apr;74(4):481–490. doi: 10.7326/0003-4819-74-4-481. [DOI] [PubMed] [Google Scholar]
- MCKENZIE J. M. Studies on the thyroid activator of hyperthyroidism. J Clin Endocrinol Metab. 1961 Jun;21:635–647. doi: 10.1210/jcem-21-6-635. [DOI] [PubMed] [Google Scholar]
- Mitsuma T., Colucci J., Shenkman L., Hollander C. S. Rapid simultaneous radioimmunoassay for triiodothyronine and thyroxine in unextracted serum. Biochem Biophys Res Commun. 1972 Mar 24;46(6):2107–2113. doi: 10.1016/0006-291x(72)90766-8. [DOI] [PubMed] [Google Scholar]
- Nicoloff J. T., Fisher D. A., Appleman M. D., Jr The role of glucocorticoids in the regulation of thyroid function in man. J Clin Invest. 1970 Oct;49(10):1922–1929. doi: 10.1172/JCI106411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Odell W. D., Wilber J. F., Utiger R. D. Studies of thyrotropin physiology by means of radioimmunoassay. Recent Prog Horm Res. 1967;23:47–85. doi: 10.1016/b978-1-4831-9826-2.50005-2. [DOI] [PubMed] [Google Scholar]
- Patel Y. C., Burger H. G., Hudson B. Radioimmunoassay of serum thyrotropin: sensitivity and specificity. J Clin Endocrinol Metab. 1971 Nov;33(5):768–774. doi: 10.1210/jcem-33-5-768. [DOI] [PubMed] [Google Scholar]
- Refetoff S., DeGroot L. J., Benard B., DeWind L. T. Studies of a sibship with apparent hereditary resistance to the intracellular action of thyroid hormone. Metabolism. 1972 Aug;21(8):723–756. doi: 10.1016/0026-0495(72)90121-7. [DOI] [PubMed] [Google Scholar]
- Refetoff S., DeWind L. T., DeGroot L. J. Familial syndrome combining deaf-mutism, stuppled epiphyses, goiter and abnormally high PBI: possible target organ refractoriness to thyroid hormone. J Clin Endocrinol Metab. 1967 Feb;27(2):279–294. doi: 10.1210/jcem-27-2-279. [DOI] [PubMed] [Google Scholar]
- Sterling K., Bellabarba D., Newman E. S., Brenner M. A. Determination of triiodothyronine concentration in human serum. J Clin Invest. 1969 Jun;48(6):1150–1158. doi: 10.1172/JCI106072. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sterling K., Brenner M. A. Free thyroxine in human serum: simplified measurement with the aid of magnesium precipitation. J Clin Invest. 1966 Jan;45(1):153–163. doi: 10.1172/JCI105320. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sterling K., Refetoff S., Selenkow H. A. T3 thyrotoxicosis. Thyrotoxicosis due to elevated serum triiodothyronine levels. JAMA. 1970 Jul 27;213(4):571–575. doi: 10.1001/jama.213.4.571. [DOI] [PubMed] [Google Scholar]
- Wilber J. F., Utiger R. D. The effect of glucocorticoids on thyrotropin secretion. J Clin Invest. 1969 Nov;48(11):2096–2103. doi: 10.1172/JCI106176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wolff J., Jones A. B. Inhibition of hormone-sensitive adenyl cyclase by phenothiazines. Proc Natl Acad Sci U S A. 1970 Feb;65(2):454–459. doi: 10.1073/pnas.65.2.454. [DOI] [PMC free article] [PubMed] [Google Scholar]