
Figure 1. Blood Tregs are not diminished in GVHD.
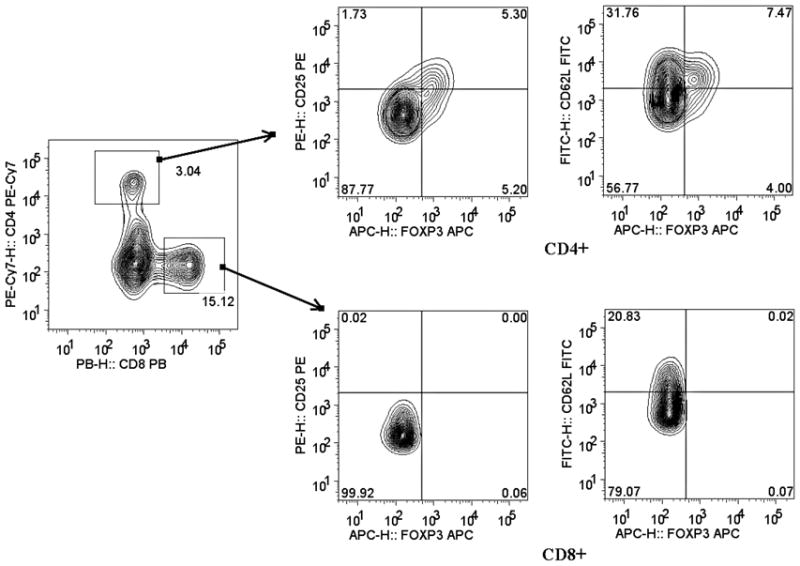
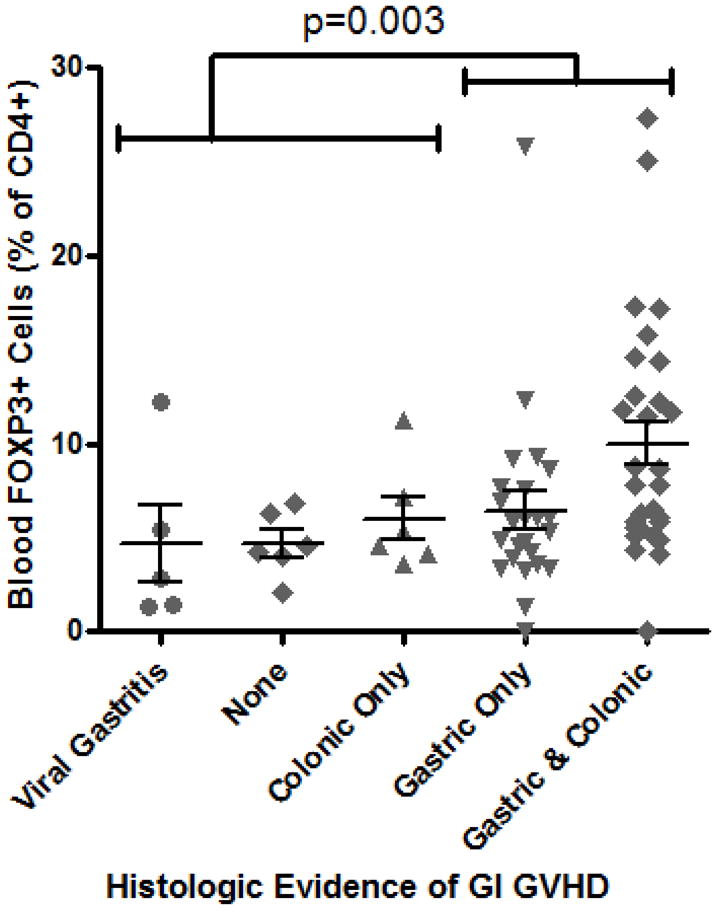
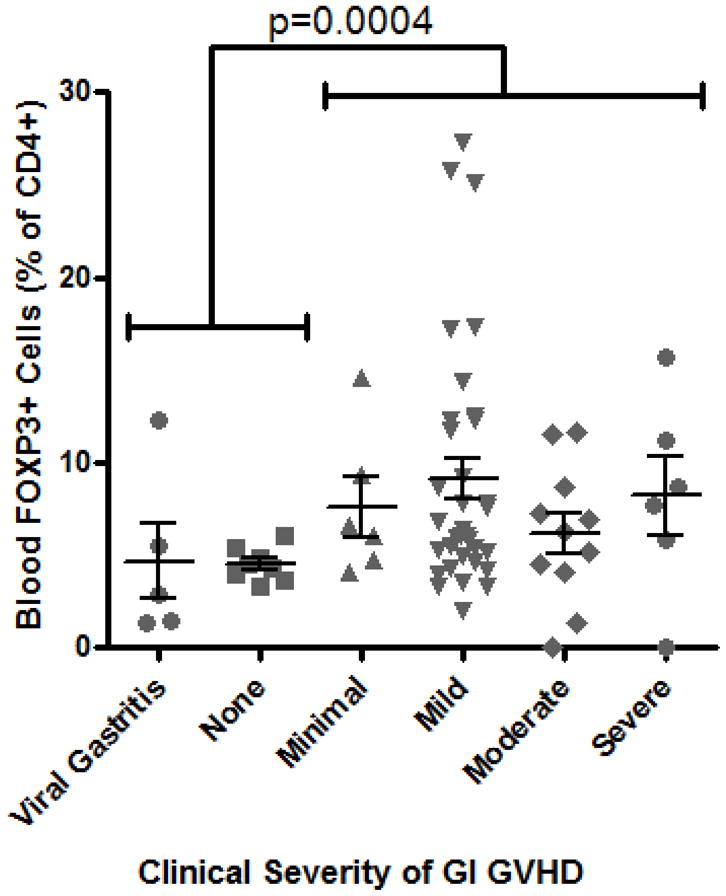
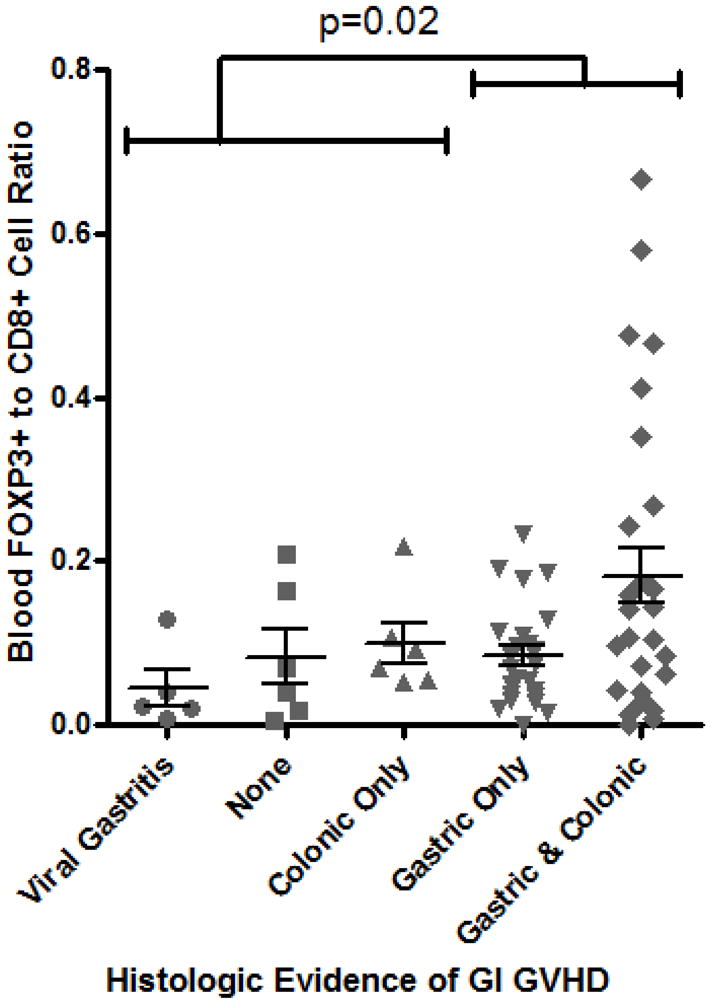
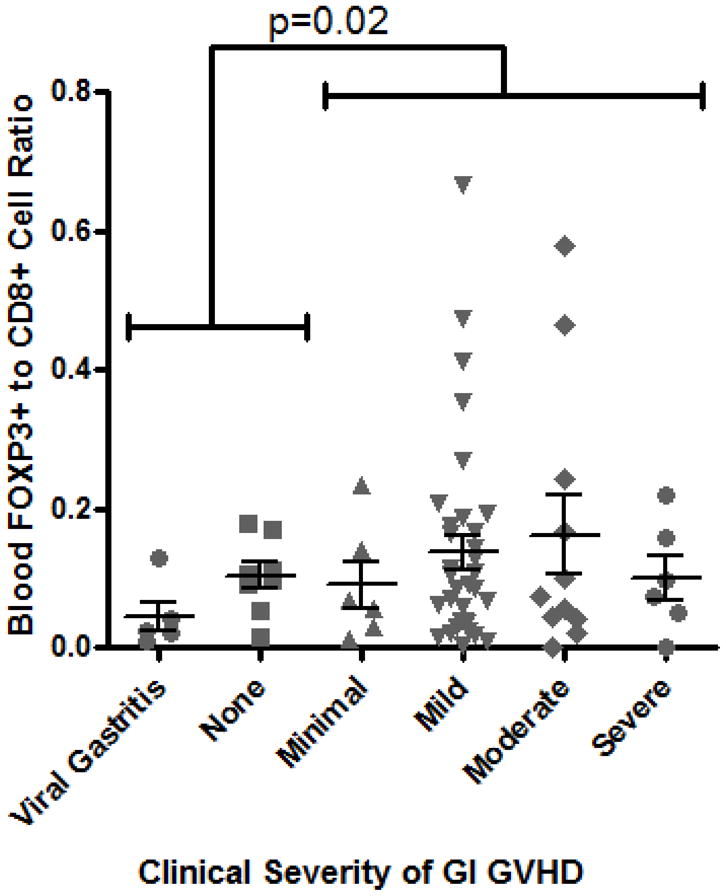
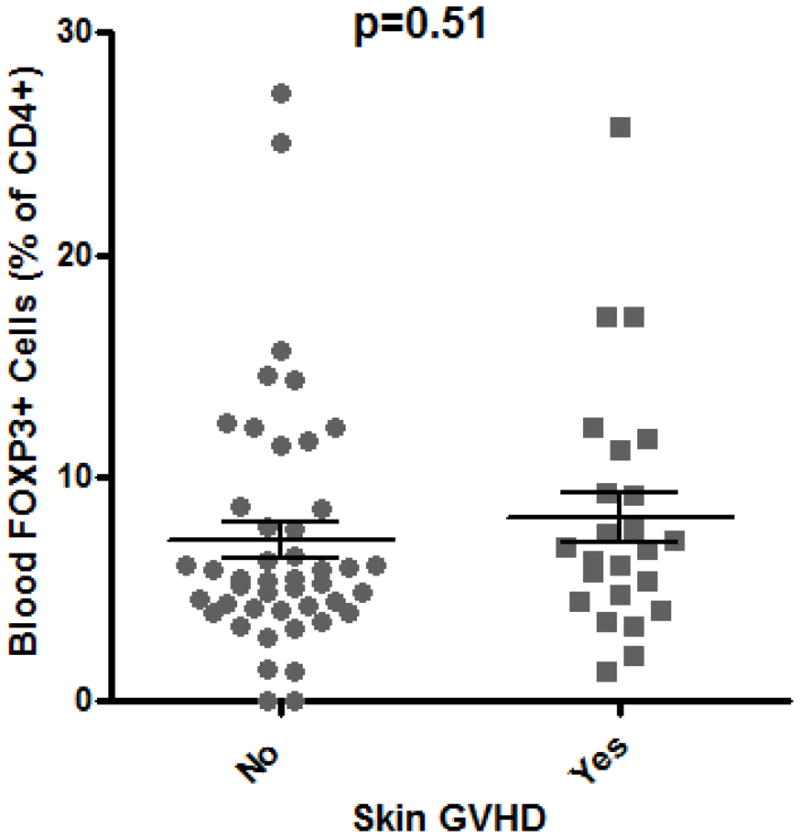
A: Representative plot of flow cytometric evaluation of blood, gated on live lymphocytes (left panel), and then gated on either CD4+ (upper panels) or CD8+ (lower panels) T cells. For each specimen, 4-quadrant gates were set to exclude >99% of cells stained with isotype control antibodies from positive quadrants (data not shown). B: The percent of CD4+ blood lymphocytes expressing FOXP3 by FACS is shown for patients with histologic evidence of GVHD in gastric biopsies (“upper GI only”), colorectal biopsies (“lower GI only”), or both (“upper & lower”) versus neither (“none”) or viral gastritis (CMV or adenovirus). The difference between all cases with versus without histologic evidence of GVHD in the stomach was analyzed to generate the p-value shown. C: FOXP3 expressing CD4+ lymphocytes were compared as in B between patients with varying clinical severity of GI GVHD, defined as described in “materials and methods”. All patients with any clinical evidence of GI GVHD were pooled for comparison with patients without clinical GI GVHD or with viral gastritis to generate the p-value shown. D, E: The ratio of blood FOXP3+ lymphocytes to CD8+ lymphocytes, determined by FACS, was compared between the cohorts described in B and C. F: FOXP3 expressing CD4+ lymphocytes were compared as in B between patients with versus without clinical evidence of skin GVHD.