
Figure 3.
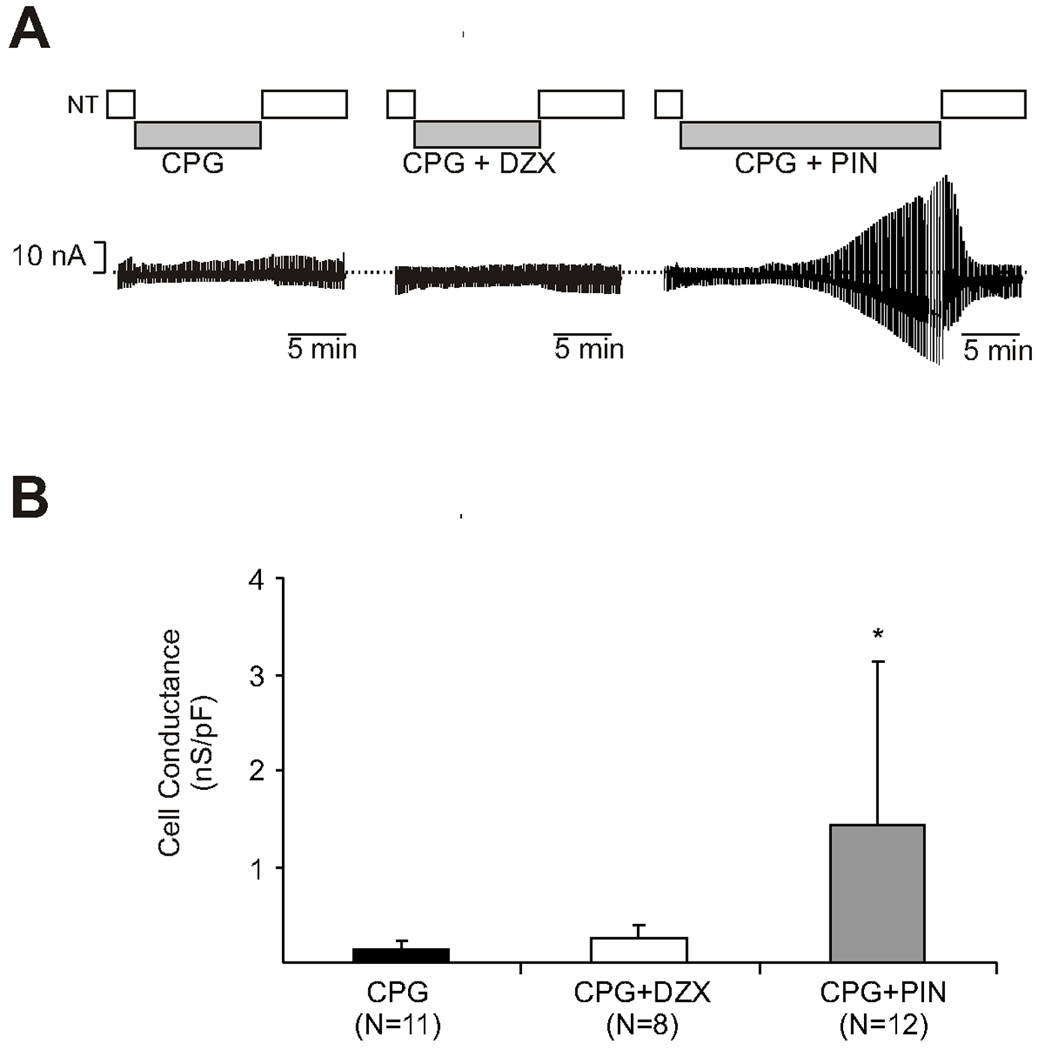
A. Pinacidil elicits an increase in adenosine triphosphate–sensitive potassium current in wild type cells exposed to cardioplegia while diazoxide does not. The y-axis represents potassium current (nA) and the x-axis represents time. Wild type myocytes were initially exposed to normal Tyrode’s solution for baseline potassium current measurement, followed by test solution, followed by reexposure to normal Tyrode’s solution. The first graph (far left) is a representative cell exposed to hyperkalemic cardioplegia (St. Thomas solution) alone during the test period. The second graph (middle) is a representative cell exposed to cardioplegia with diazoxide during the test period. The third graph (far right) is a representative cell exposed to cardioplegia with pinacidil during the test period. The addition of pinacidil to cardioplegia induced potassium current. CPG is hyperkalemic cardioplegia, DZX is diazoxide, NT is normal Tyrode’s solution, and PIN is pinacidil.
B. Pinacidil elicits an increase in adenosine triphosphate–sensitive potassium current in wild type cells exposed to cardioplegia while diazoxide does not. Cell conductance is represented in nanoseimens/picofarads (nS/pF, y axis) and test solution on the x axis. Test solutions included: hyperkalemic cardioplegia (St. Thomas solution), cardioplegia with diazoxide, and cardioplegia with pinacidil. When correcting for cell conductance, there was a significant increase in potassium current in cells exposed to pinacidil supplemented cardioplegia (*p= 0.025 vs. CPG). CPG is cardioplegia, DZX is diazoxide, PIN is pinacidil, and N is number of myocytes.