
Figure 6.
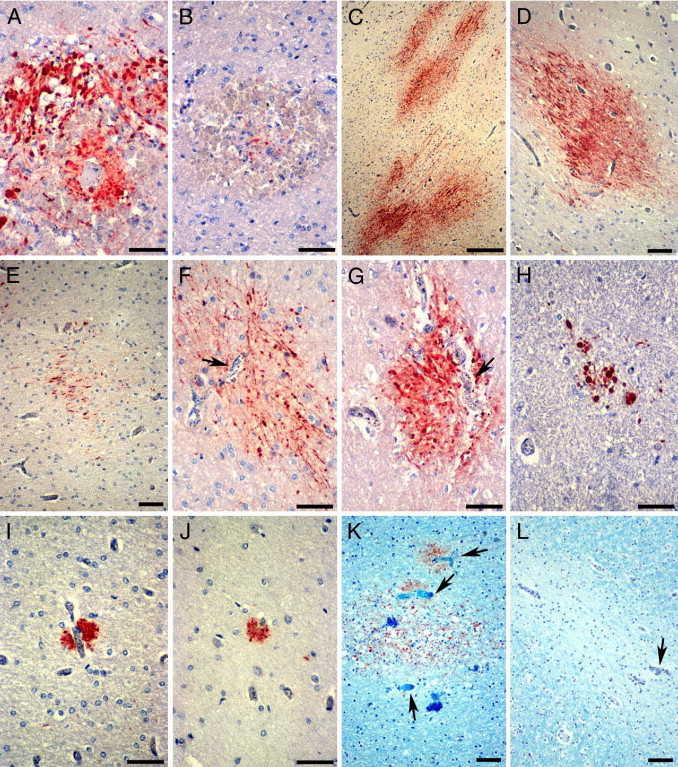
Patterns of axonal damage in pediatric CM detected by β-APP IHC. A and B: RH-associated axonal damage. A: Strongly β-APP–immunoreactive swollen and disrupted axons in an RH around a thrombosed and ruptured white matter capillary. B: Only a few β-APP–positive axons are present in the center of some RHs. C through H: Diffuse axonal injury in CM2 patients. Confluent (C) or single (D) ill-defined irregular patches of β-APP–immunoreactive axons in the cerebral and cerebellar white matter (C, E, and F), the gray-white matter junction (D), and pons (G). Diffuse axonal damage occurs in areas with heavy iRBC sequestration (F and G, arrows). H: Smaller diffuse lesions are evident in the medulla. I and J: Small discrete foci of β-APP–positive axons are present immediately adjacent to capillaries occluded by iRBC with (I) or without (J) a thrombus. In sections double stained for β-APP and Luxol fast blue, diffuse axonal and myelin lesions often (K), but not invariably (L), coincide in areas with prominent iRBC sequestration (arrows). Scale bars: 50 μm (A, B, and F–J); 250 μm (C); 100 μm (D, E, K, and L).