
Figure 3.
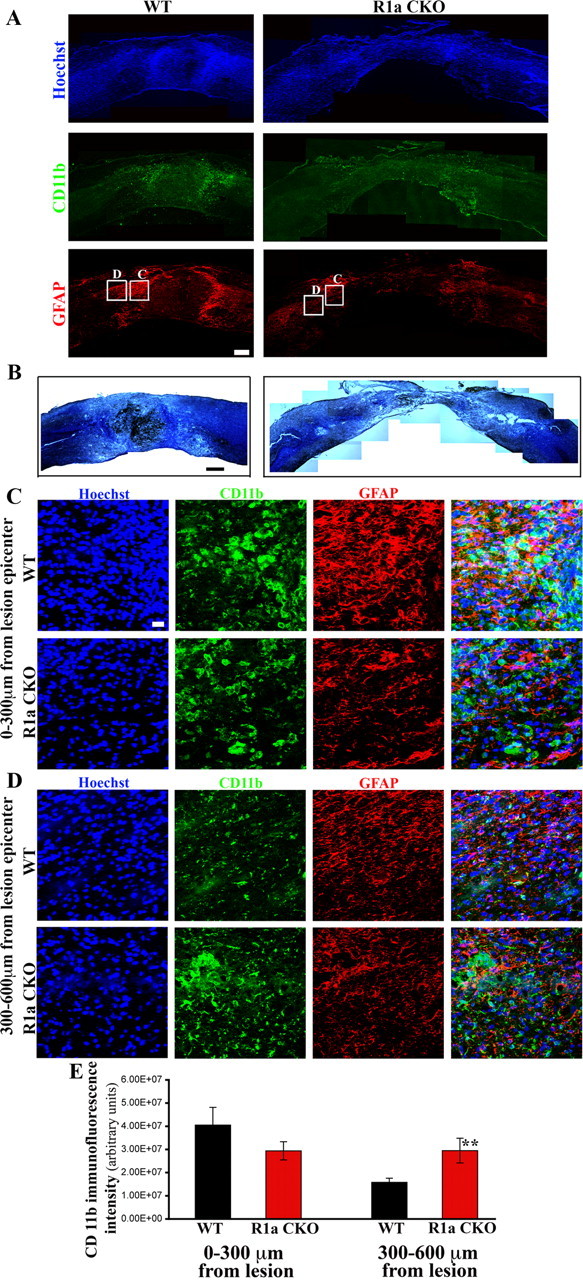
BMPR1a conditional knock-out mice show defective gliosis and increased inflammatory infiltration after spinal cord injury. A, Injured spinal cords at 1 week postinjury from BMPR1a WT and CKO mice. Rostral is to the left and dorsal to the top of the images. WT cords show intense GFAP+ astrocytes (red) staining at the edge of the lesion, a sign of reactive gliosis, that is not observed in the BMPR1a CKO mice. The astrocytes in the WT mice have condensed the CD11b-positive inflammatory cells(green) toward the lesion (intense green seen in and around the GFAP stain while these are still present diffusely in the parenchyma in the BMPR1a CKO mice. (Scale bar: 200 μm). B, WT and BMPR1a CKO spinal cords stained with a modified Weigert protocol (see Materials and Methods) and counterstained with cresyl violet showing greater tissue loss in BMPR1a CKO animals. (Scale bar: 250 μm). C, Higher-magnification (40×) images taken from the boxed regions shown in A. Note that there is intense CD11b staining in this area in the WT mice and the astrocytes have extended long processes. The astrocytes in the BMPR1a CKO mice have smaller, thinner processes. D, Images (40×) of boxed regions in A taken in the region spanning 300–600 μm from the edge of the lesion. Note the increased CD11b staining that persists in this area in the BMPR1a CKO mice that is comparable to the levels seen in C. Scale bars (C, D), 20 μm. Blue, Hoechst; green: CD11b; red, GFAP. E, Quantification of the CD11b staining intensity in the regions described in B and C in WT and BMPR1a CKO mice. There is a significantly higher CD11b staining in the region 300–600 μm from the lesion edge. (n = 3 WT and BMPR1a CKO animals **p < 0.0039 by Student's unpaired t test).