

Abstract
The reconstruction of large uncontained defects represents a major challenge to the revision total knee surgeon, and the outcome of the revision often depends on the management of these bone deficiencies. We report the first successful use of both complete distal femoral and proximal tibia massive allografts in the reconstruction of large femoral and tibial uncontained defects during revision total knee arthroplasty. At the five-year follow up, we did not find any infection, graft failure or loosening of implant, in spite of using two massive structural allografts in a single revision total knee arthroplasty.
Keywords: Massive allograft, revision total knee arthroplasty, uncontained bone defect
INTRODUCTION
Failure of a total knee arthroplasty (TKA) is often associated with loss of bone from either the proximal aspect of tibia or the distal aspect of the femur. These defects are usually classified as contained or uncontained.1 The reconstruction of large uncontained defects represents a major challenge to the revision surgeon. Options for reconstruction2 of large defects include metal augments, custom prostheses, massive autogenous bone-grafts and massive allografts. Use of cement is appropriate only for contained defects. Metal augments are recommended only for small to medium sized defects in elderly low demand patients. Custom prostheses are costly, time consuming to manufacture and may not fit as well as planned or at all at the time of surgery. Autogenous bone-grafting is not suitable for large defects or in situations where structural support is required.
Allografts provide a biological solution, have the advantage of easy fashioning to fit irregular defects, restore bone stock and have relatively low cost. Use of femoral head allograft, complete distal femur or proximal femur allograft has been reported in some studies3,4 ; however, no study has reported use of both distal femur and proximal tibia allograft in a single revision total knee arthroplasty.
We report the first successful use of both complete distal femoral and proximal tibia massive allografts in the reconstruction of large femoral and tibial uncontained defects during revision total knee arthroplasty.
CASE REPORT
A 70-year-old male patient, farmer by occupation, presented with a swollen, painful and unstable right knee with primary complaint of inability to bear weight. Passive range of motion was painful and limited to 10 degrees of hyperextension to 50 degrees of flexion in April 2005. Primary TKA for osteoarthritis was performed 12 years back in some other hospital. The patient also had a periprosthetic supracondylar fracture of femur following a trivial fall, for which open reduction and internal fixation was done elsewhere eight years back with condylar blade plate. The skin revealed thick scar tissue on both anterior and lateral aspects of the knee due to secondary wound healing after previous surgeries. Anteroposterior and lateral radiographs [Figure 1] revealed severe osteolytic bone defects on femoral and tibial aspects along with primary total knee prosthesis and condylar blade plate in situ. Infection was ruled out preoperatively with bone scan and laboratory markers (Erythrocyte sedimentation rate, C- Reactive Protein). We decided to reconstruct the knee with structural distal femur and proximal tibia allografts and constrained fixed-bearing revision knee prosthesis (Nexgen, LCCK, Zimmer, Warsaw).
Figure 1.

Anteroposterior and lateral X-rays of right knee showing extensive osteolysis on both femoral and tibial aspects
Operative technique
We used the previous midline incision and a medial parapatellar approach. We removed much necrotic, granulomatous tissue (biopsy proven) which usually occurs due to extensive polyethylene wear. Total knee prosthesis was found loose and removed easily. We were also able to remove the condylar blade plate through the same approach.
After debridement, the whole proximal tibia [Figure 2] presented a massive uncontained defect, classified as type III according to Anderson Orthopaedic Research Institute classification.5 The whole distal femur also presented a large uncontained type III bone defect involving both medial and lateral femoral condyles [Figure 2]. The medial collateral ligament attachment on the femoral side was saved. However, femoral attachment of lateral collateral ligament was deficient, and ligament was identified with a piece of bone.
Figure 2.
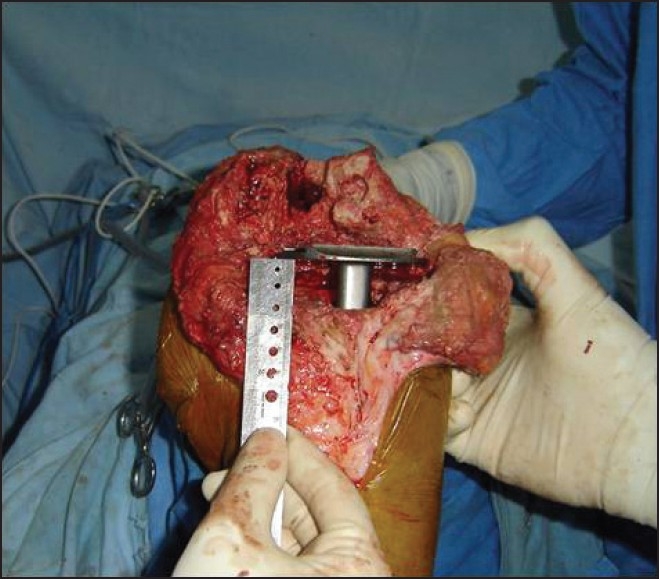
The intraoperative photograph shows the defect after thorough debridement
Both proximal tibial and distal femoral cadaveric allografts [Figure 3] with a diameter smaller than that of the host bone were selected so that they could be placed within the host cortical shell. The allografts were taken from our own cadaveric bone bank, where they underwent radiation with 2.5 megarads and were stored at –70°C. Two surgical teams were used during the management of the case, for optimal efficiency. One team prepared the allograft, making appropriate femoral cuts and cementing in a long-stemmed revision femoral component. The other surgical team prepared the recipient bone. Cultures were taken from the knee as well as the allograft to rule out any existing infection.
Figure 3.

Step-cut prepared distal femoral and proximal tibial allografts
Both the recipient distal femur and proximal tibia were step-cut with minimal bone resection. On the side table, step-cut was made in both allografts to match that of the host bone and instrumented with trial implants. The implant allograft composite was put for trial in situ, and the cuts were fine tuned as required. Soft tissues were balanced to obtain equal flexion and extension gaps.
After trial, the revision knee components were cemented [Figure 4] on the back-table into the distal femoral and proximal tibial allografts with a long stem. Care was taken during cementing to avoid getting cement on the interface between the graft and the host. Once the cement had set, the construct was implanted with full assembly, matching the two step-cuts. The residual host femur, with its ligaments and other soft tissues attached, was wrapped around the allograft host junction to serve as a living bone graft [Figure 5]. Lateral collateral ligament was attached with the help of two screws. Extensor mechanism alignment and tracking was checked, and the wound was closed in layers.
Figure 4.

Fully prepared composite allograft with LCCK implant
Figure 5.
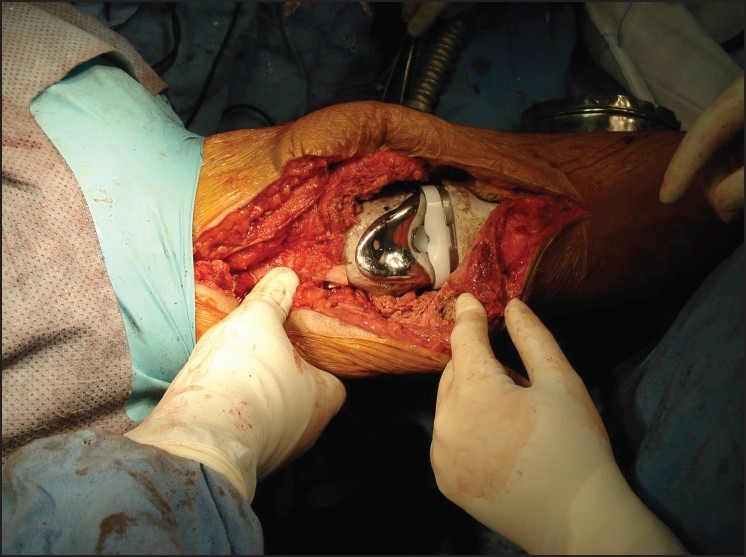
Intraoperative photograph showing invagination of composite allografts into host bone
Follow up
Prophylactic antibiotics consisted of an intravenous first-generation cephalosporin for five days, followed by oral antibiotics for seven days. Gentle active and passive ranges of motion were begun at 48 hours. Partial weight bearing was allowed at four weeks, and full weight bearing was started after eight months when there was radiographic evidence of union on both sides. No wound complication was noted during the entire follow up.
At the end of five years of follow up (i.e., in April 2010), the patient was walking full weight bearing and had complete incorporation of allograft and host bone with no signs of osteolysis [Figure 6]. His active range of motion range of motion (ROM) was 0-110 degrees.
Figure 6.

Anteroposterior and lateral X-rays of the same patient at five-year follow-up showing good allograft incorporation
DISCUSSION
Few options are available to the surgeon for reconstruction of massive bone defects surrounding a failed total knee arthroplasty (TKA). The application of allografts in revision TKA is an attractive option. The use of femoral head allografts for the management of large bone defects in revision TKA has been reported. Very few studies have also reported using either massive distal femoral or proximal tibial allograft for large defect reconstruction in revision TKA.3,4
Our patient presented a unique problem, having severe bone loss on both femoral and tibial aspects. Using both massive distal femoral and proximal tibial allografts proved to be a successful mode of treatment with distinct advantages. Placing the allograft within the vascularized host bone will add some structural support to the allograft and provide an environment by which the allograft may eventually incorporate.
One major concern with the use of allografts is the risk of infection. In a large series by Lord et al.,6 the risk of infection with the use of small allografts (femoral heads) was negligible; and with the use of larger allografts, acceptable (4%-5%). Some authors have recommended plate and screw fixation of the allograft in addition to invagination of the graft, to ensure rotational stability. Using a stemmed component and avoiding the use of plate fixation decreases the need for extensive soft tissue dissection, avoids weakening of the graft and may decrease the risk of infection by preserving the soft tissue envelope.7
Another concern about the use of massive allografts is their performance in the long term, especially in view of reports showing resorption and failures of allografts used in revision total hip arthroplasty at longer follow ups. However, use of allografts in anatomically matching sites (proximal tibia for proximal tibia, distal femur for distal femur) allows for accurate orientation of trabeculae along the lines of stress. This may lessen the likelihood of early mechanical failure. This technique requires that the allograft is appropriately shaped for intussusception into the host bone with stable struts of host bone maximally contacting step-cuts in the graft.8
The limitation in terms of applicability of this study in practice could be the non-availability of such allografts at many centers. Newer trabecular metal wedges and sleeves may be an option; however, they are very costly. These allografts are free for patients at our institute and provide a biological and effective alternative. There should be a stimulus to establish more and more cadaveric allograft retrieval centers to deal with the complex and often neglected cases of bone loss, which is particularly common in the Indian scenario.
The use of dual structural massive allografts provides a stable and durable reconstruction of this uncommon presentation with both femoral and tibial large bone deficiencies encountered during a revision TKA. At a five-year follow-up, we did not find any infection, graft failure or loosening of implant, in spite of using two massive structural allografts in a single revision TKA. Further follow up with large number of patients is necessary to determine the long term fate of these allografts.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Stockley I, McAuley JP, Gross AE. Allograft reconstruction in total knee arthroplasty. J Bone Joint Surg Br. 1992;74:393–7. doi: 10.1302/0301-620X.74B3.1587885. [DOI] [PubMed] [Google Scholar]
- 2.Mow CS, Wiedel JD. Structural allografting in revision total knee arthroplasty. J Arthroplasty. 1996;11:235–41. doi: 10.1016/s0883-5403(96)80072-6. [DOI] [PubMed] [Google Scholar]
- 3.Backstein D, Safir O, Gross A. Management of bone loss: Structural grafts in revision total knee arthroplasty. Clin Orthop Relat Res. 2006;446:104–12. doi: 10.1097/01.blo.0000214426.52206.2c. [DOI] [PubMed] [Google Scholar]
- 4.Engh GA, Ammeen DJ. Use of structural allograft in revision total knee arthroplasty in knees with severe tibial bone loss. J Bone Joint Surg Am. 2007;89:2640–7. doi: 10.2106/JBJS.F.00865. [DOI] [PubMed] [Google Scholar]
- 5.Engh GA. Revision total knee arthroplasty. Baltimore: Williams and Wilkins; 1997. Bone defect classification; pp. 63–120. [Google Scholar]
- 6.Lord CF, Gebhardt MC, Tomford WM, Mankin HJ. Infection in bone allografts.Incidence, nature, and treatment. J Bone Joint Surg Am. 1988;70:369–76. [PubMed] [Google Scholar]
- 7.Bezwada HP, Shah AR, Zambito K, Cerynik DL, Johanson NA. Distal femoral allograft reconstruction for massive osteolytic bone loss in revision total knee arthroplasty. J Arthroplasty. 2006;21:242–8. doi: 10.1016/j.arth.2005.06.005. [DOI] [PubMed] [Google Scholar]
- 8.Zatsepin ST, Burdygin VN. Replacement of the distal femur and proximal tibia with frozen allografts. Clin Orthop Relat Res. 1994;303:95–102. [PubMed] [Google Scholar]