
Figure 2. Three potential mechanisms for hyperkalemia in patients of PHA2 with WNK4 mutations.
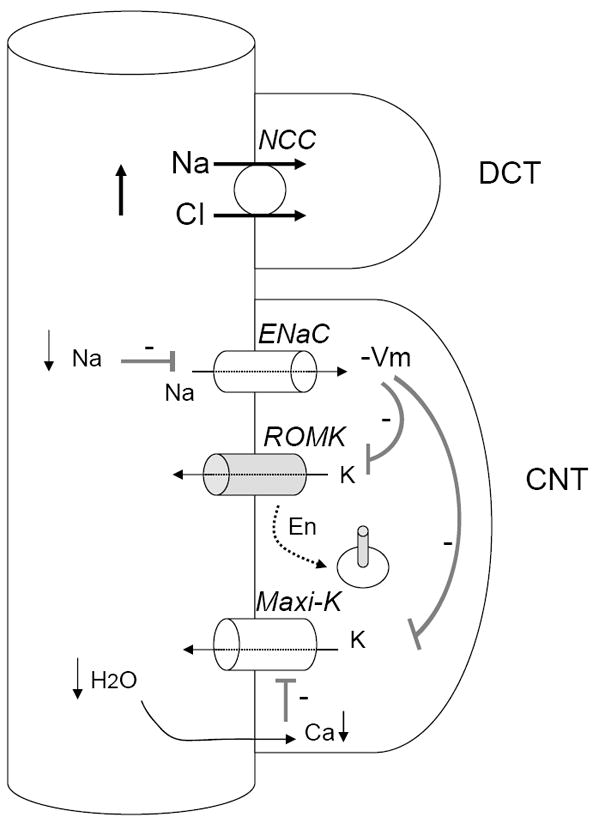
First, overactivity of NCC decreases Na+ reabsorption via ENaC, hyperpolarizes membrane potential (indicated by “-Vm”), and decreases K+ efflux via ROMK and maxi-K. Second, mutations in WNK4 that cause PHA2 inhibit ROMK by increasing its endocytosis (indicated by “En”). Third, reduced fluid flow to CNT decreases the opening of maxi-K. Because hyperkalemia causes upregulation of ROMK and maxi-K, the increase in the endocytosis of ROMK and “functional” inhibition of maxi-K (i.e., secondary to reduced Na+ and fluid delivery) are likely critical for sustained hyperkalemia.