
Figure 3. Hypothetical model for steady-state tubular Na+ handling in PHA2 patients with WNK4 mutations.
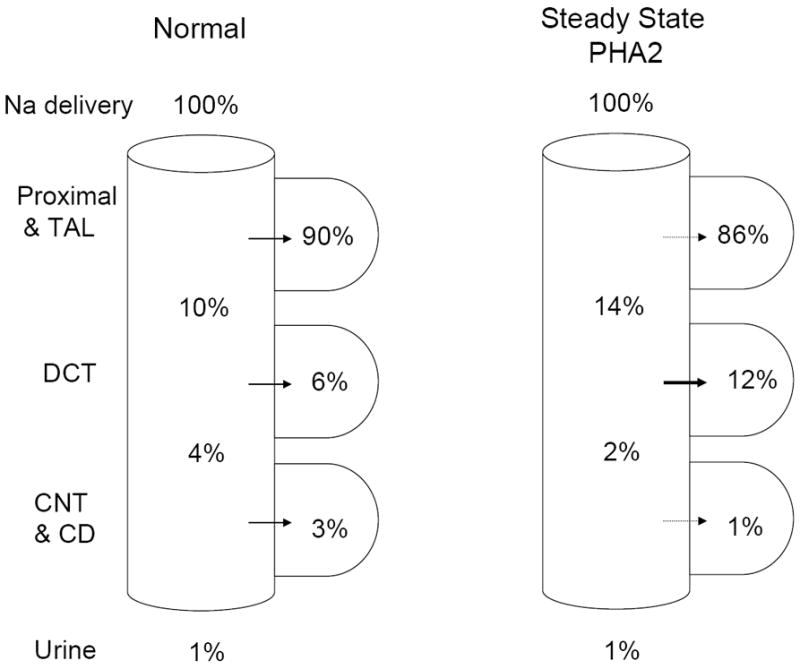
It is assumed that WNK4 mutations increase Na+ reabsorption in DCT from 6% (of filtered load) in control to 12% in the diseased state. Assuming that the compensatory decrease in Na+ reabsorption (in response to volume expansion and hypertension) occurs in the tubular segments proximal as well as distal to DCT, Na+ delivery to the CNT/CD will be reduced compared to the control (2% vs 4% in PHA2 vs control, respectively). It should be mentioned that the axial fluid profile does not parallel that for Na+ delivery because DCT lacks aquaporin-2.