

Abstract
Morality may be innate to the human brain. This review examines the neurobiological evidence from research involving functional magnetic resonance imaging of normal subjects, developmental sociopathy, acquired sociopathy from brain lesions, and frontotemporal dementia. These studies indicate a “neuromoral” network for responding to moral dilemmas centered in the ventromedial prefrontal cortex and its connections, particularly on the right. The neurobiological evidence indicates the existence of automatic “prosocial” mechanisms for identification with others that are part of the moral brain. Patients with disorders involving this moral network have attenuated emotional reactions to the possibility of harming others and may perform sociopathic acts. The existence of this neuromoral system has major clinical implications for the management of patients with dysmoral behavior from brain disorders and for forensic neuropsychiatry.
INTRODUCTION
For years, scientists and philosophers have proposed a sixth human sense for morality. Recently, there is increasing evidence that there is, in fact, an intrinsic morality network. The presence of a moral sense is consistent with a focus of human evolution on mechanisms of individual behavior that maximize survival in social groups. Evolution has promoted social cooperation through emotions against harming others, a need for fairness and the enforcement of moral rules, empathy and “Theory of Mind” (ToM), as well as other behaviors that feed into the concept of morality. ToM is the ability to appreciate the thoughts, feelings, and beliefs of others.
If there is a “moral sense,” then there should be specific brain mechanisms for morality as well as brain disordered patients with impaired morality. Convergent evidence that this is the case comes from studies of functional magnetic resonance imaging (fMRI) in normals, neurological investigations of sociopaths, and the examination of patients with focal brain lesions or with frontotemporal dementia (FTD). This neurobiological evidence points to an automatic, emotionally- mediated moral network that is centered in the ventromedial prefrontal cortex (VMPFC), particularly in the right hemisphere. Although this literature is still young, disparate, and heavily reliant on fMRI correlations, the convergence of evidence supports the presence of a neuromoral brain network. This report reviews this burgeoning literature and discusses the theoretical implications for brain-behavior relationships, and its clinical and legal implications. Although much of the presented evidence is still debated, a picture of moral neuroscience is beginning to emerge.
MORALITY: DEFINITION AND BACKGROUND
Morality is a code of values and customs that guide social conduct. An example of a moral value is the avoidance of harm to others (“no-harm” rule). Philosophers often divide morality into “descriptive” or “normative” types. Descriptive morality is a code of conduct held by a particular society or group as authoritative in all matters of right and wrong. It focuses on areas beyond no-harm, such as purity, accepting authority, and emphasizing loyalty to the group.1 Normative morality, on the other hand, is a universal code of moral actions and prohibitions held by all rational people, irregardless of their society or group’s descriptive morality.1,2 It focuses predominantly on no-harm and fairness but also includes the other aspects of morality. Philosophers since pre-Socratic times have long pondered the existence of a universal normative morality in addition to the descriptive codes proposed by each society, religion, or legal system.
Neurobiology is concerned with normative morality, which can lead to different codes of moral behavior when it interacts with socio-cultural learning.2–4 The interface of evolutionary psychology with social neuroscience points to universal “neuromoral” emotions and drives that strengthen social cohesion and cooperation. 5,6 Studies with apes and other social animals describe moral emotions such as empathy, gratitude, a sense of fairness, feelings of reciprocity, righteousness, consolation, and group loyalty.7–9 In humans, moral emotions, such as guilt, shame, embarrassment, gratitude, compassion, pride, fear of negative evaluation by others, and outrage at unfair treatment, are strong motivators to act in a socially favorable way.10,11 These emotions or sentiments allow humans to quickly grasp the moral implications of social interactions and then act to enhance their personal reputations and the likelihood of future social cooperation.12 Furthermore, moral emotions are manifestations of evolutionary-based neuromoral drives including no-harm, fairness or equity, community, authority, and purity.1,13 The two most prominent of these may be no-harm, as evidenced by the discomfort felt on directly hurting others,14 and fairness, as evidenced by the need to punish “free-riders” or those who cheat and break the rules.15
PSYCHOLOGICAL AND fMRI STUDIES IN NORMALS
Investigators have used fMRI in normals to define the neuroanatomy of moral behavior.4,14,16 These studies usually involve tasks or dilemmas of moral judgment or reasoning.14,16–19 The main neuromoral areas involved are the VMPFC and adjacent orbitofrontal, plus ventrolateral, cortex (OFC/VL), amygdalae, and the dorsolateral prefrontal cortex (DLPFC) (Figure 1).4,5,14,16,18 The VMPFC (defined here as Brodmann’s areas [BA]10–12, 25, 32 plus the frontopolar region of BA10) attaches moral and emotional value to social events, anticipates their future outcomes, and participates in ToM, empathy, attribution of intention, and related tasks.20–23 The OFC/VL region (defined here as BA47, parts of BA10–12 and 25, plus VL BA44), mediates socially aversive responses, changes responses based on feedback, and inhibits impulsive, automatic, or amygdalar responses.24–26 The amygdalae, located in the anteromedial temporal lobes, mediate the response to threat and aversive social and moral learning.6,27,28 The DLPFC can override this neuromoral network through the application of reasoned analysis to moral situations. 18 Finally, some fMRI morality and related tasks activate additional regions such as the anterior insula,29 posterior superior temporal sulcus (pSTS),30–32 anterior cingulate gyrus,33 the inferior parietal lobules and temporoparietal junctions,32,34–36 ventral striatum and mesolimbic reward system,37 precuneus,35 and posterior cingulate.30,32 Other regions, such as subcortical limbic and anterior temporal lobes, can lead to impaired moral behavior as well.5,38
FIGURE 1. Anatomic areas in morality network.
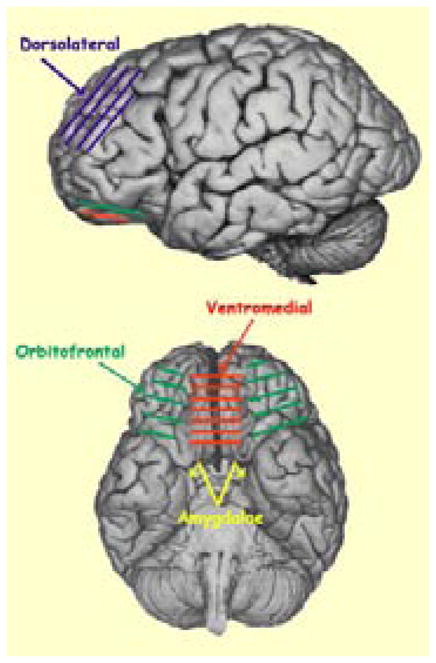
Originally from Thebrain.mcgill.ca, “copyleft” permission.
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
The VMPFC, particularly on the right, is core to this neuromoral system. In fMRI studies, this brain region becomes activated with tasks requiring explicit moral judgments, passive viewing of morally salient photos (Figure 2), and the elicitation of charity, fairness, guilt, and other moral emotions and sentiments.16,22,30,39 Greene and colleagues14 have found VMPFC activation on presenting “personal” moral dilemmas involving the possibility that the participant’s direct action could cause someone serious harm (Table 1), compared to “impersonal” moral dilemmas where the possibility of causing someone serious harm does not involve the participant’s direct action on another. These findings indicate that the VMPFC mediates automatic moral and “prosocial” reactions, such as discomfort at the prospect of being a direct agent of a personal moral violation or of harm to someone else.40–42 In fact, fMRI studies indicate that the VMPFC participates in prosocial, affiliative, or social attachment emotions in general, including guilt, embarrassment, and compassion. 22,43,44 In contrast, Greene and colleagues14 have found DLPFC activation on presentation of the impersonal moral dilemmas, suggesting a later, dispassionate, reasoned, or cost-benefit assessment for moral judgments in the absence of a sufficient VMPFC “moral reaction.”8,18,30,45–50
FIGURE 2. Ventromedial prefrontal cortex in moral judgment and emotion16.
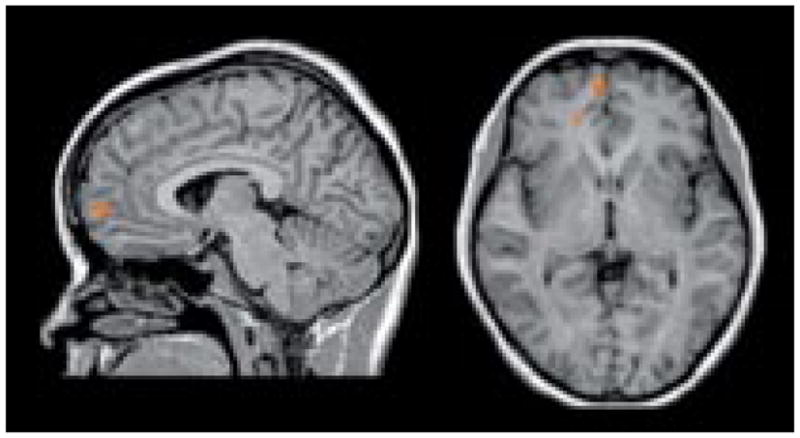
Activation in response to passive exposure to morally salient pictures compared to emotionally salient non-moral pictures.
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
TABLE 1.
Example of Reasoned and Personal Moral Dilemmas14
| Reasoned moral dilemmas included the following: |
| 1. Standard Trolley: Imagine that you are at the wheel of a runaway trolley quickly approaching a fork in the tracks. On the tracks going to the left is a group of five railway workmen. On the tracks going to the right is a single railway workman. If you do nothing, the trolley will proceed to the left, causing the deaths of the five workmen. The only way to avoid the deaths of these workmen is to hit a switch on your dashboard that will cause the trolley to proceed to the right, causing the death of the single workman. Would you hit the switch in order to avoid the deaths of the five workmen? |
| 2. Resume: You have a friend who has been trying to find a job for a long time but without success. He has a family to support and he is desperate. It occurs to him that he would be more likely to get a job if he just had a more impressive resume. He decided to put some false information on his resume in order to make it more impressive. By doing this he ultimately got a job, beating out several other more qualified candidates. Was it ok for your friend to put false information on his resume in order to help him get the job? |
| 3. Taxes: You are the owner of a small business worried about surviving, making ends meet, and paying your taxes. It occurs to you that you can lower your taxes by pretending that some of your personal expenses are business expenses. For example, you could pretend that the stereo in your home is being used in your business office or that your dinners out with your wife are dinners with clients. Is it ok for you to report personal expenses as business expenses in order to survive and make ends meet? |
| 4. Standard Fumes: You are the night watchman in a hospital. There is an accident and deadly fumes in the ventilation system are traveling to the hospital rooms. In one room there are three patients. In another room there is a single man. If you do nothing the fumes will go into the room with the three patients and kill them. The only way to avoid this is to hit a switch that will reroute the fumes into the other room with the single man, killing him instead. Is it appropriate for you to hit the switch in order to avoid the deaths of the three patients? |
| 5. Lost Wallet: You are walking down the street when you come across a wallet lying on the ground. You open the wallet and find that it contains several hundred dollars in cash. From the credit cards and other items in the wallet, it’s clear that it belongs to a very wealthy man. You, on the other hand, are very poor and need money. You consider sending the wallet back to the owner without the money, keeping the money for yourself. Would you keep the money you found in the rich man’s wallet? |
| Personal moral dilemmas included the following: |
| 1. Footbridge: Imagine that a runaway trolley is heading down the tracks toward five workment who will be killed if the trolley keeps going. You are on a footbridge over the tracks in between the approaching trolley and the five workmen. Next to you on this footbridge is a stranger who happens to be very large. The only way to save the lives of the five workmen is to push this stranger off the bridge and onto the tracks below where his large body will stop the trolley. The stranger will die if you do this, but the five workmen will be saved. Would you to push the stranger onto the tracks in order to save the five workmen? |
| 2. Transplant: You are a doctor. You have five patients, each of whom is about to die due to a failing organ of some kind. You have another patient, a young man who is healthy. The only way that you can save the lives of the first five patients is to transplant five of this young man’s organs (against his will) into the bodies of the other five patients. If you do this, the young man will die, but the other five patients will live. The families and staff beg you to do this. Would you refuse their requests to do the transplants that would save five of your patients? |
| 3. Smother for dollars: You are in the hospital visiting a sick friend. A young man sitting next to you is visiting his very sick father who has only a week to live. He tells you that his father has a large life insurance policy that runs out at midnight. If his father dies before midnight, this young man gets millions of dollars. The money would mean a great deal to him and he sees no value in his father’s suffering for a few more days. He offers you a million dollars to go up to his father’s room and smother his father with a pillow. Would you to smother this man’s father in order to get money for yourself and this young man? |
| 4. Crying Baby: Enemy soldiers have taken over your village. They have orders to kill everyone. You have hidden in the basement of a large house along with other people. Outside you hear the voices of soldiers who have come to search the house. Your baby begins to cry loudly. You cover his mouth to block the sound. If you remove your hand from his mouth the soldiers will hear his crying and will kill you, your baby, and the other people hiding in the basement. To save yourself and the others you must smother your child to death. Would you smother your child in order to save yourself and the other people? |
| 5. Modified Lifeboat: You are on a cruise ship when there is a fire on board and the ship has to be abandoned. Unfortunately, the lifeboat that you get in has too many people and may sink. Your lifeboat is beginning to fill with water. If nothing is done your lifeboat will sink before the rescue boat arrives and everyone may die. However, there is a seriously injured person in the lifeboat. The other passengers ask you to help them throw that person overboard so that the lifeboat will not sink. Would you refuse to help the others throw this person overboard in order to save as many passengers as possible? |
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
In addition to emotions to do no harm, moral emotions serve to enforce moral rules by attributing negative intentions and seeking to punish “cheaters” who violate them.15,44,51 This “altruistic punishment” is a manifestation of the moral drive for fairness and equity. There is increased VMPFC activation from a sense of fairness (Figure 3), which contributes to the drive to punish violators or non-cooperators, even if costly for the punisher.44.51,52 This is further exemplified in the Ultimatum Game, where one player must divide a sum of money with a second player, but if the second player rejects the division as unfair, neither player receives anything. The second player’s rejection of unfair offers, and the foregoing of any money whatsoever, usually reflects both their sense of fairness and desire for altruistic punishment.53 Altruistic punishment is strongly dependent on determining that others, particularly those with a negative reputation, are deliberately not playing by the rules.44,54 The VMPFC is involved through its role in attribution or in inferring the intention of others’ behavior. 55 The OFC/VL (BA47) region and neighboring anterior insula and amygdala, especially on the right,52,56 subsequently effect altruistic punishment through sentiments linked to social aversion/exclusion, such as anger, indignation, disgust, and contempt.22,43,44,57–61
FIGURE 3. fMRI study of fairness52.
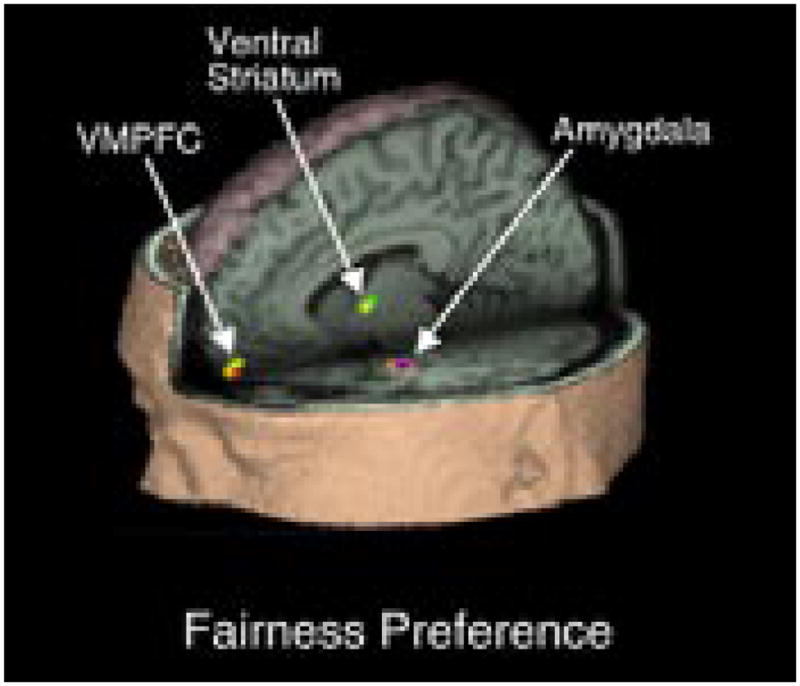
VMPFC activation, along with ventral striatum and amygdala, associated with fairness preference. The illustration shows the location of clusters with significantly greater activation in response to fair compared with unfair offers.
VMPFC=ventromedial prefrontal cortex.
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
ToM and empathy are two processes very closely related to morality. ToM involves the VMPFC, which facilitates the appreciation that others have thoughts, feelings, and beliefs.33,62,63 The “cognitive” aspects of empathy, such as taking someone else’s perspective and vicariously identifying with it, involve the VMPFC (BA10,11) in a phylogenetically new system that only occurs in great apes and advanced mammals.42,64–68 The most emotional aspects of empathy, such as emotional contagion, include the OFC/VL (BA44) in a phylogenetically old system.64,65,69–71 Variables that strongly affect “cognitive” empathy, and impact on VMPFC (BA10) activity, include the self as the agent of an action and the perceived similarity between the self and others.58,72 This suggests that the VMPFC deals with complex “self-other conjoining,” or a resonating of the protagonist’s mental and emotional states with that of someone else. Other areas modulate self-other conjoining, including OFC/VL mirror neurons, when observed intentions and emotions of others are internally mapped or imitated;65,73–82 the anterior cingulate cortex, when self-concepts are threatened by the outperformance of others (envy);33 and the ventral striatum, when pleasure results from another’s misfortune (“schadenfreude”).33
DEVELOPMENTAL SOCIOPATHY
Neuroscience has come a long way since the claims of an innate “criminal mind” from Cesare Lombroso and others.83 Neuroimaging and other techniques have revealed a great deal about the neurobiology of morality through the study of sociopathy, or chronic antisocial behavior. Sociopaths lack moral emotions, empathy, conscience, or remorse and guilt for their acts. Although they have difficulty distinguishing between moral (victim-based) transgressions and conventional (social disorder-based), they have normal moral knowledge and reasoning.60,61 Sociopaths have instrumental (cold-blooded and goal-directed) aggression with decreased sympathetic arousal. On psychophysiological measures, they show minimal alterations in heart rate, skin conductance, or respirations when they are subjected to fear or stressful or unpleasant pictures, and they have reduced autonomic responses to the distress of others, as well as reduced recognition of sad and fearful expressions.84–86
Those who have committed violent offenses have a high incidence of neurological changes. In one study, nearly two-thirds of murderers had neurological diagnoses, including brain injuries, mental retardation, cerebral palsy, epilepsy, dementia, and others.87 Neurological examinations often show marked frontal or temporal deficits or changes on neuroimaging or electroencephalography.88 Some of these deficits could be due to alcohol or substance abuse or other confounding variables, and future studies will need to control for these variables. Deficits in frontal functions such as inability to change their responses (response reversal learning) or to inhibit risk-taking behavior after negative feedback occur among institutionalized and violence-prone patients.60,89–94 Functional neuroimaging studies can show frontotemporal hypometabolism, hypoperfusion, or changes in spectroscopy in murderers pleading not guilty by reason of insanity and in violent psychiatric inpatients.86,88,89,95–98 Voxel-based morphometry reveals a correlation of frontopolar and OFC/VL grey matter reduction with increased psychopathic traits or scores.98,99 A reduction in prefrontal gray matter volume associated with reduced autonomic arousal occurs among violent offenders.100 Moreover, the smaller the volume of prefrontal cortex, the greater the tendency towards sociopathic behavior is among known sociopaths.101 Paradoxically, boys with callous unemotional conduct problems have increased gray matter concentrations in medial frontal regions, suggesting a delay in cortical maturation.102
In addition to the predominant frontal lobe abnormalities, sociopaths have reduced function of the amygdalae.60,103 These structures are involved in aversive or fear conditioning, instrumental learning (reward), and the retrieval of socially relevant knowledge, such as facial trust-worthiness, approachability, or fear.27 Sociopaths are impaired in these and in anticipatory stimulus- reinforcement learning,104 information which is needed by the VMPFC for the development of normal moral socialization.60,61,105 Animal studies further show that the early amygdalar dysfunction disrupts the appropriate development of the VMPFC and the OFC/VL.60,105 In developmental sociopathy, early amygdalar dysfunction may result in VMPFC and OFC/VL dysfunction, through the impaired association of actions that harm others with the aversive reinforcement of the victims’ distress. Finally, there is evidence for subtle changes in a whole network of areas in developmental psychopathy.98
ACQUIRED SOCIOPATHY IN LESION STUDIES
Ever since the descriptions of Phineas Gage, perhaps neurology’s most famous patient, clinicians have viewed patients with VMPFC lesions as characterized by alterations in social and moral behavior (Figure 4). Focal lesions affecting VMPFC and adjacent OF/VLC include strokes, trauma, tumors, infections, and a ruptured anterior commissure aneurysm.83,106 Right frontal lesions may be especially associated with deviant social behavior and left frontal lesions associated with violent or angry outbursts.83,107,108 Consistent with other data, investigations show that focal lesions in the VMPFC and OFC/VL impair moral judgment, and early lesions of these areas impair the development of moral knowledge and judgment. 109,110 When VMPFC lesions are acquired before 16 months of age, they may lead to severe antisocial behavior, insensitivity to future consequences of decisions, and repeated failure to respond to behavioral interventions.109
FIGURE 4. Phineas Gage’s skull.
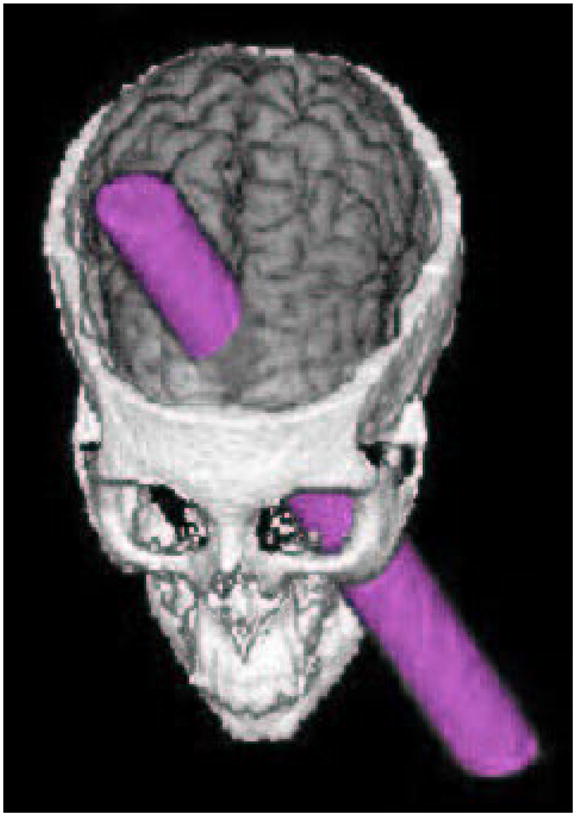
On September 13, 1848, while working with explosives, an explosion sent a rod through Phineas Gage’s skull. The rod traversed the ventromedial prefrontal cortex region and altered his moral and social behavior.
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
The lesions implicated in “acquired sociopathy” involve the VMPFC and the OFC/VL. Patients with focal VMPFC lesions, especially on the right, have attenuated feelings of emotional discomfort for sociomoral violations, severe deficits in empathy, and reduced responsiveness to victims.9,22,68,89,110–120 VMPFC lesions, especially on the right, disturb “fortune-of-others” and related emotions such as compassion, shame, guilt, envy, inappropriate pride, and gloating; emotions that correlate with perspective-taking and ToM.109,116,117,121–124 Although first-order ToM may be intact, they may be particularly unable to read the feelings and emotions (“affective ToM”) of others as evident on irony and faux pas tasks.118,125 Like developmental sociopaths, patients with VMPFC lesions had autonomic hyporesponsivity, especially in response to social stimuli,66,100,116,120 but compared to developmental sociopaths, their hyporesponsivity is more general and not selective for fearful or sad expressions.126,127 They also differ in that patients with VMPFC lesions do not crave constant stimulation, and they are not deceitful, manipulative, or instrumentally aggressive.59 Finally, OFC/VL lesions impair the use of immediate feedback from social and emotional cues, and the control of emotional and impulsive responses.24,57,59,60,128
Several recent research studies have used moral dilemmas to investigate moral decision-making among patients with VMPFC lesions. Ciaramelli and colleagues114 compared 7 patients with VMPFC lesions with 12 normal controls on personal, impersonal, and non-moral dilemmas. Compared to normal controls, the patients were significantly more willing to judge personal moral violations as acceptable behaviors, and they did so quickly and with little hesitation. In a similar study, Koenigs and colleagues117 carefully examined six patients with focal bilateral damage to the VMPFC (Figure 5). Their patients maximized the good for the many (utilitarianism) on moral dilemmas, had impaired autonomic activity in responses to emotionally charged pictures, and had diminished empathy, embarrassment, and guilt. In both of these studies, compared to controls, the patients with VMPFC damage tend to make utilitarian choices in conflicting moral dilemmas.114,117 In contrast, patients with VMPFC lesions may continue to reject unfair offers in the Ultimatum Game,129 a finding that suggests that their intact OFC/VL region, with relatively preserved socially aversive sentiments,22 continues to apply altruistic punishment in situations where fairness and intentionality are overt or predefined.12,22 The sparing of the VL areas related to aversion may add to the emotional negative aspects of their behavior and render them vehement self-centered moralists.12,114
FIGURE 5. Ventromedial prefrontal cortex in moral judgment and emotion117.

Top: Group lesion mapping medial views of the right and left hemispheres. The VMPFC was damaged in all patients; the overlap between different patients is shown by the coloring.
Bottom: Lesions of the six VMPFC patients displayed in mesial views and coronal slices. The color bar indicates the number of overlapping lesions at each voxel.
VMPFC=ventromedial prefrontal cortex.
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
Despite their deficits in per sonal moral responses, patients with adult-onset VMPFC lesions retain moral knowledge and reasoning. Although early-onset VMPFC lesions can impair the acquisition of moral knowledge,109,110 patients with adult-onset VMPFC lesions have preserved moral reasoning and retain the knowledge of moral rules and conventions.129–132 On moral tasks, they can verbalize the differences between right and wrong responses, but they may not act on that knowledge and can score well on self-report moral behavioral inventories (Table 2). In sum, patients with VMPFC lesions do not act according to their retained moral knowledge because they have a deficit in prosocial or affiliative sentiments, and do not use their moral reasoning abilities to anticipate the future consequences, outcomes, or feelings of their actions.10–12,22,112,113,133–137 One reason for this partially retained moral knowledege is that it is located outside the VMPFC, particularly in the right anterior temporal lobe.43
TABLE 2. Moral Behavior Inventory150.
This questionnaire presents acts for you to evaluate in terms of right or wrong. Please answer to the best of your ability. Choose 1 if the item seems not wrong. Choose 4 if the item seems Severely Wrong. Use 2 for Mildly Wrong and 3 for Moderately Wrong.
| How wrong is it if you: |
| _____ Fail to keep minor promises |
| _____ Take the last seat on a crowded bus |
| _____ Sell someone a defective car |
| _____ Drive after having one drink |
| _____ Cut in line when in a hurry |
| _____ Don’t give blood during blood drives |
| _____ Are mean to someone you don’t like |
| _____ Say a white lie to get a reduced fare |
| _____ Drive out the homeless from your community |
| _____ Always let others pay at a restaurant |
| _____ Not help someone pick up their dropped papers |
| _____ Keep over-change at a store |
| _____ Not offer to help after an accident |
| _____ Ignore a hungry stranger |
| _____ Fail to vote in minor elections |
| _____ Keep money found on the ground |
| _____ Temporarily park in a handicap spot |
| _____ Cut off drivers on the freeway |
| _____ Take the largest piece of a pie |
| _____ Falsely get out of jury duty |
| _____ Ask others do some of your homework |
| _____ Take credit for others’ work |
| _____ Refuse to help people who don’t deserve it |
| _____ Get more time off than your co-workers |
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
FTD AND DISEASE STATES
Brain disorders including slow, insidious neurodegenerative dementias, are another window to the organization of morality in the brain. There are many brain disorders that can disturb sociomoral behavior, such as Huntington’s disease, traumatic brain injury, frontal tumors and other conditions (Table 3). Perhaps the most characteristic is FTD. This disease can serve as a model to illustrate alterations in moral behavior from brain diseases.
TABLE 3.
Neurological Diseases with Potential Disturbances of Moral Behavior
| 1. Frontotemporal lobar degenerations, eg, frontotemporal dementia |
| 2. Huntington’s disease |
| 3. Autism spectrum disorders |
| 4. William’s syndrome |
| 5. Traumatic brain injury |
| 6. Epilepsy |
| 7. Strokes and other focal lesions in frontotemporal regions |
| 8. Other frontally predominant dementias, eg, Alzheimer’s variant, vascular dementia |
| 9. Other inheritable disorders: Down’s syndrome, Prader-Willi and Angleman syndromes, Turner syndrome, fragile X syndrome |
| 10. Anoxic encephalopathy |
| 11. Infections: Creutfeldt-Jakob disease, HIV, Neurosyphilis |
| 12. Hydrocephalus |
| 13. Parkinson plus disorders |
| 14. Tumors, eg, butterfly glioma of the frontal lobes |
| 15. Demyelinating disorders, eg, multiple sclerosis, metachromatic leukodystrophy |
| 16. Motor neuron disease with frontotemporal dementia |
| 17. Toxins and alcohol |
| 18. Non-infectious encephalopathies, eg, paraneoplastic, Hashimoto’s, steroid-responsive |
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
In contrast to the memory and cognitive deficits of Alzheimer’s disease and other dementias, the core features of FTD are transgression of social norms including sociopathic behavior, a loss of empathy or appreciation of the feelings of others, and a loss of insight for their behavior and its consequences.138 In FTD, asymmetric right-sided frontal involvement is especially associated with socially undesirable behaviors, loss of empathy, and a distorted appreciation of others. 139–143 FTD patients manifest violations of social and moral rules or norms early in their disease.138 Most commonly there is a loss of social tact and propriety, unacceptable physical contact, and improper verbal or nonverbal communication.144 Sociopathic behavior occurs in more than half of patients with FTD (Table 4).145 Investigators have described FTD patients with stealing and shoplifting, 145–147 inappropriate sexual behavior,138,148 physical aggression and acts of violence,146,148 frequent traffic violations and hit-and-run accidents,148 pedophilia,149 and other transgressions.145 These sociopathic acts are associated with right frontal, presumably VMPFC, involvement on imaging and on neuropathology.143,144
TABLE 4.
Sociopathic Acts Among 16 Patients with Frontotemporal Dementia145
| Number | Type |
|---|---|
| 3 | Unsolicited sexual approach or touching |
| 3 | Traffic violations including hit-and-run accidents |
| 2 | Physical assaults |
| 1 | Shoplifting |
| 1 | Deliberate non-payment of bills |
| 1 | Pedophilia |
| 1 | Indecent exposure in public |
| 1 | Urination in inappropriate public places |
| 1 | Stealing food |
| 1 | Eating food in grocery store stalls |
| 1 | Breaking and entering into others’ homes |
Mendez MF. CNS Spectr. Vol 14, No 11. 2009.
Early FTD affects the VMPFC more than the DLPFC, and studies show corresponding impairments of emotionally-based moral judgments. In one study, FTD patients were impaired in their ability to immediately respond to personal moral dilemmas, compared to Alzheimer’s disease patients and normal controls.150 Using relatively intact DLPFC processes, the FTD patients solved the moral dilemmas in a logical, cold, and calculating fashion. These patients have problems with empathy, both empathic concern and perspective taking.136 Investigations of personality among FTD patients have also shown decreased empathy and decreased agreeableness with right OFC/VL involvement and inter-personal coldness or decreased emotional empathy with anterior temporal involvement.151–154 On voxel-based morphometry studies, empathy correlates with a right medial frontotemporal network (VMPFC and anterior temporal areas).151,155 FTD patients are particularly impaired in gauging the seriousness of moral transgressions.136 Other studies document defects in ToM in patients with FTD,125,136,156–158 as well as deficits in social concepts from right anterior temporal lobe involvement.43
In FTD, defective moral emotions along with decreased self-other conjoining could account for defective moral judgment as well as most of their observed sociopathic acts. There is a selective impairment in decision-making in personal moral judgment in FTD in the face of relatively preserved moral knowledge and moral reasoning ability.150 Their impersonal responses to personal moral violations are consistent with the early focus of neuropathology in the VMPFC.144 These changes, coupled with insufficient control of impulsivity from adjacent OFC/VL involvement, explain the tendency to impulsive moral violations in full knowledge of the potential consequences. Furthermore, involvement of the rigth anterior temporal in FTD can lead to social knowledge deficits and contribute to the moral behavioral changes in this disorder.43,151
DISCUSSION
The evidence from fMRI studies in normals, sociopathy, brain lesions, and FTD suggest a neuromoral network of prosocial emotions and drives that promote social cohesiveness and cooperation.1,6,159 Most moral judgments are rapid, involuntary, and intuitive; whereas, deliberate rational reasoning is often post hoc rationalization for judgments which have already occurred.8,13,45 Normative morality appears to be rooted in an intrinsic neuromoral network.
The neuromoral network comprises the VMPFC, especially on the right, the OFC/VL, the amygdalae, and related structures.16 The VMPFC, with its rich interconnections with limbic structures, mediate these strong automatic reactions to moral violations.4,14,16,18,45,81 Brain lesions or diseases that involve the right VMPFC reduce moral emotions and responses to dilemmas that involve either harm to others or a sense of fairness or equity. The OFC/VL region manages socially aversive emotions and may inhibit immediate and amygdalar responses, suppresses impulsive behavior, and responds to feedback learning.24,59 The amygdalae mediate the response to immediate threat, aversive social learning, and help incorporate social or moral prohibitions.27 Some investigators also propose that this morality network can be over-ridden by DLPFC-mediated reasoning processes, resulting in utilitarianism, ie, the greatest good for the greatest many.22
If the brain has a “moral grammar,” it is less in the Chomsky sense than in an interaction of moral drives with the process of self-other conjoining. 160,161 Biological moral drives, such as no-harm and fairness, are the forces that result in moral emotions. In the VMPFC, this is coupled with automatic, complex self-other conjoining. The result is the creation of joint attention and “intersubjective space,”162 ie, the activation of one’s representations of the state and situation of others.8,76 Unless actively inhibited, activation of these shared representations probably occurs automatically through mirror neurons and results in ToM, empathy, moral emotions, and moral behavior.163–167
These new findings have implications for clinical neuropsychiatry. Patients may present with alterations in moral behavior due to brain disorders. They can manifest as shoplifting, hit-and-run accidents, lack of empathic aid, or the spectrum from subtle changes in personality all the way to serious crimes like pedophilia.149 When patients present with dysmoral behavior for the first time, as a change from a prior pervasive pattern of behavior, clinicians need to consider a possible, causative brain disorder (Table 3). Family and friends need education as to the significance of the patient’s behavior, and the question of whether their dysmoral behavior is their “fault” may need frank discussion. Lastly, medications can be useful in controlling related behaviors such as impulsivity, but do not selectively suppress dysmoral behavior. Selective serotonin reuptake inhibitors, beta-blockers, and mood stabilizing antiepileptic agents (such as valproate, carbamazepine, and lamotrigine) could be of help in this regard.
The neurobiology of morality raises additional questions of legal culpability. Patients with VMPFC lesions or FTD with disturbed volition have committed crimes and been arrested.145,146,148 The US federal insanity defense hardens the original M’Naughton rule, requiring the defendant to prove, by “clear and convincing evidence,” that “at the time of the commission of the acts constituting the offense, the defendant, as a result of a severe mental disease or defect, was unable to appreciate the nature and quality or the wrongfulness of his acts” (18 U.S.C. § 17).168 Without the restraint of intuitive moral emotions and self-other conjoining, however, patients may not be able to deter an impulse to act in an unacceptable manner, even as they know right and wrong and understand the nature of their acts. Furthermore, Anglo-American jurisprudence distinguishes between reason-based law and a natural law based on what a “reasonable person” would do in like circumstance.169 Paradoxically, under the law a “reasonable person” is someone who actually responds to intact moral emotions; therefore, the proof that these patients lack the faculties of a “reasonable person” is the sociopathic behaviors themselves. These considerations demand a reappraisal of the how we view culpability and criminal violations among brain-injured patients.83
Of necessity, this review summarizes a large number of studies that are disparate in their scope and variable in their approach. Most published studies focus on social behavior, rather than specifically on moral behavior. The case for a neuromoral network is primarily based on cross-sectional studies correlating fMRI findings with either task performance or with clinical characteristics supplemented by developmental and acquired sociopathy, and findings from patients with FTD. As a result, the conclusions from this review require future hypothesis-driven studies with specific causal inferences.
CONCLUSION
Current research is beginning to outline a neuromoral network with a hub in the VMPFC. This research has implications for understanding the organization of our moral sense in the brain and has implications for clinical and forensic neuropsychiatry. The findings reviewed here are preliminary, but this story promises to rapidly unfold as more research is done on the neurobiological basis of morality in normals and in brain-injured patients.
FOCUS POINTS.
Humans have an innate moral sense based in a neuromoral network centered in the ventromedial prefrontal cortex and its connections.
The neuromoral network works through moral emotions and moral drives, such as the avoidance of harm to others and the need for fairness and punishment of violators; it includes self-other conjoining processes, such as Theory of Mind and empathy, which also involve the ventromedial prefrontal cortex.
Disorders of this region, such as focal lesions or frontotemporal dementia, disturb personal, intrinsic moral emotions and decision-making.
Clinicians must recognize and manage “acquired sociopathy” and other dysmoral behaviors associated with disorders of the neuromoral network.
Patients with these disorders pose a special problem for forensic neuropsychiatry.
Acknowledgments
Funding/Support: This work was supported by grant #R01AG034499-02.
Footnotes
Faculty Disclosures: Dr. Mendez reports no affiliations with or financial interest in any organiztion that may pose a conflict of interest.
References
- 1.Haidt J. The new synthesis in moral psychology. Science. 2007;316:998–1002. doi: 10.1126/science.1137651. [DOI] [PubMed] [Google Scholar]
- 2.Wilson JQ. The Moral Sense. New York, NY: Simon & Schuster; 1993. [Google Scholar]
- 3.Hauser MD. Moral Minds: How Nature Designed our Universal Sense of right and Wrong. New York, NY: Ecco/Harper Collins; 2006. [Google Scholar]
- 4.Moll J, de Oliveira-Souza R, Eslinger PJ. Morals and the human brain: a working model. Neuroreport. 2003;14:299–305. doi: 10.1097/00001756-200303030-00001. [DOI] [PubMed] [Google Scholar]
- 5.Moll J, Zahn R, de Oliveira-Souza R, Krueger F, Grafman J. Opinion: the neural basis of human moral cognition. Nat Rev Neurosci. 2005;6:799–809. doi: 10.1038/nrn1768. [DOI] [PubMed] [Google Scholar]
- 6.Berthoz S, Grezes J, Armony JL, Passingham RE, Dolan RJ. Affective response to one’s own moral violations. Neuroimage. 2006;31:945–950. doi: 10.1016/j.neuroimage.2005.12.039. [DOI] [PubMed] [Google Scholar]
- 7.De Waal FB. How animals do business. Sci Am. 2005;292:54–61. [PubMed] [Google Scholar]
- 8.Haidt J. The emotional dog and its rational tail: A social intuitionist approach to moral judgment. Psychol Rev. 2001;108:814–834. doi: 10.1037/0033-295x.108.4.814. [DOI] [PubMed] [Google Scholar]
- 9.Hauser MD, Cushman FA, Young LL. A dissociation between moral judgments and justifications. Mind Language. 2006;22:1–21. [Google Scholar]
- 10.Fiske AP. Moral emotions provide the self-control needed to sustain social relationships. Self Identity. 2002;1:169–175. [Google Scholar]
- 11.Tangney JP, Stuewig J, Mashek DJ. Mirror neuron system: basic findings and clinical applications. Ann Neurol. 2007;62:213–218. doi: 10.1002/ana.21198. [DOI] [PubMed] [Google Scholar]
- 12.Moll J, Schulkin J. Social attachment and aversion in human moral cognition. Neurosci Biobehav Rev. 2009;33:456–465. doi: 10.1016/j.neubiorev.2008.12.001. [DOI] [PubMed] [Google Scholar]
- 13.Pinker S. The New York Times Magazine. Jan 13, 2008. The moral instinct. [Google Scholar]
- 14.Greene JD, Sommerville RB, Nystrom LE, Darley JM, Cohen JD. An fMRI investigation of emotional engagement in moral judgment. Science. 2001;293:2105–2108. doi: 10.1126/science.1062872. [DOI] [PubMed] [Google Scholar]
- 15.Cosmides L, Tooby J, Fiddick L, Bryant GA. Detecting cheaters. Trends Cogn Sci. 2005;9:505–506. doi: 10.1016/j.tics.2005.09.005. [DOI] [PubMed] [Google Scholar]
- 16.Moll J, Oliveira-Souza R, Eslinger PJ, et al. The neural correlates of moral sensitivity: a functional magnetic resonance imaging investigation of basic and moral emotions. J Neurosci. 2002;22:2730–2736. doi: 10.1523/JNEUROSCI.22-07-02730.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Schaich Borg J, Hynes C, Van Horn J, Grafton S, Sinnott-Armstrong W. Consequences, action, and intention as factors in moral judgments: an FMRI investigation. J Cogn Neurosci. 2006;18:803–817. doi: 10.1162/jocn.2006.18.5.803. [DOI] [PubMed] [Google Scholar]
- 18.Greene JD, Nystrom LE, Engell AD, Darley JM, Cohen JD. The neural bases of cognitive conflict and control in moral judgment. Neuron. 2004;44:389–400. doi: 10.1016/j.neuron.2004.09.027. [DOI] [PubMed] [Google Scholar]
- 19.Heekeren HR, Wartenburger I, Schmidt H, Schwintowski HP, Villringer A. An fMRI study of simple ethical decision-making. Neuroreport. 2003;14:1215–1219. doi: 10.1097/00001756-200307010-00005. [DOI] [PubMed] [Google Scholar]
- 20.D’Argembeau A, Xue G, Lu ZL, Van der Linden M, Bechara A. Neural correlates of envisioning emotional events in the near and far future. Neuroimage. 2008;40:398–407. doi: 10.1016/j.neuroimage.2007.11.025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Damasio AR. Descartes’ Error: Emotion, Reason, and the Human Brain. New York, NY: Putnam; 1994. [Google Scholar]
- 22.Moll J, de Oliveira-Souza R. Moral judgments, emotions and the utilitarian brain. Trends Cogn Sci. 2007;11:319–321. doi: 10.1016/j.tics.2007.06.001. [DOI] [PubMed] [Google Scholar]
- 23.Moll J, De Oliveira-Souza R, Zahn R. The neural basis of moral cognition: sentiments, concepts, and values. Ann NY Acad Sci. 2008;1124:161–180. doi: 10.1196/annals.1440.005. [DOI] [PubMed] [Google Scholar]
- 24.Baxter MG, Parker A, Lindner CC, Izquierdo AD, Murray EA. Control of response selection by reinforcer value requires interaction of amygdala and orbital prefrontal cortex. J Neurosci. 2000;20:4311–4319. doi: 10.1523/JNEUROSCI.20-11-04311.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Roelofs K, Minelli A, Mars RB, van Peer J, Toni I. On the neural control of social emotional behavior. Soc Cogn Affect Neurosci. 2009;4:50–58. doi: 10.1093/scan/nsn036. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Rolls ET, Hornak J, Wade D, McGrath J. Emotion-related learning in patients with social and emotional changes associated with frontal lobe damage. J Neurol Neurosurg Psychiatry. 1994;57:1518–1524. doi: 10.1136/jnnp.57.12.1518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Adolphs R, Tranel D, Damasio AR. The human amygdala in social judgment. Nature. 1998;393:470–474. doi: 10.1038/30982. [DOI] [PubMed] [Google Scholar]
- 28.Luo Q, Nakic M, Wheatley T, Richell R, Martin A, Blair RJ. The neural basis of implicit moral attitude–an IAT study using event-related fMRI. Neuroimage. 2006;30:1449–1457. doi: 10.1016/j.neuroimage.2005.11.005. [DOI] [PubMed] [Google Scholar]
- 29.Hsu M, Anen C, Quartz SR. The right and the good: distributive justice and neural encoding of equity and efficiency. Science. 2008;320:1092–1095. doi: 10.1126/science.1153651. [DOI] [PubMed] [Google Scholar]
- 30.Harenski CL, Hamann S. Neural correlates of regulating negative emotions related to moral violations. Neuroimage. 2006;30:313–324. doi: 10.1016/j.neuroimage.2005.09.034. [DOI] [PubMed] [Google Scholar]
- 31.Singer T, Kiebel SJ, Winston JS, Dolan RJ, Frith CD. Brain responses to the acquired moral status of faces. Neuron. 2004;41:653–662. doi: 10.1016/s0896-6273(04)00014-5. [DOI] [PubMed] [Google Scholar]
- 32.Robertson D, Snarey J, Ousley O, et al. The neural processing of moral sensitivity to issues of justice and care. Neuropsychologia. 2007;45:755–766. doi: 10.1016/j.neuropsychologia.2006.08.014. [DOI] [PubMed] [Google Scholar]
- 33.Takahashi H, Lato M, Matsuura M, Mobbs D, Suhara T, Okubo Y. When your gain is my pain and your pain is my gain: Neural correlates of envy and schadenfreude. Science. 2009;323:937–939. doi: 10.1126/science.1165604. [DOI] [PubMed] [Google Scholar]
- 34.Frith CD, Frith U. The neural basis of mentalizing. Neuron. 2006;50:531–544. doi: 10.1016/j.neuron.2006.05.001. [DOI] [PubMed] [Google Scholar]
- 35.Young L, Saxe R. The neural basis of belief encoding and integration of moral judgment. Neuroimage. 2008;40:1912–1920. doi: 10.1016/j.neuroimage.2008.01.057. [DOI] [PubMed] [Google Scholar]
- 36.Young L, Cushman F, Hauser M, Saxe R. The neural basis of the interaction between theory of mind and moral judgment. Proc Nat Acad Sci. 2007;104:8235–8240. doi: 10.1073/pnas.0701408104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Schaefer A, Collette F, Philippot P, et al. Neural correlates of “hot” and “cold” emotional processing: a multilevel approach to the functional anatomy of emotion. Neuroimage. 2003;18:938–949. doi: 10.1016/s1053-8119(03)00009-0. [DOI] [PubMed] [Google Scholar]
- 38.Zahn R, Moll J, Krueger F, Huey ED, Garrido G, Grafman J. Social concepts are represented in the superior anterior temporal cortex. Proc Nat Acad Sci. 2007;104:6430–6435. doi: 10.1073/pnas.0607061104. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Decety J, Jackson PL. The functional architecture of human empathy. Behav Cogn Neurosci Rev. 2004;3:71–100. doi: 10.1177/1534582304267187. [DOI] [PubMed] [Google Scholar]
- 40.Heekeren HR, Wartenburger I, Schmidt H, Prehn K, Schwintowski HP, Villringer A. Influence of bodily harm on neural correlates of semantic and moral decision-making. Neuroimage. 2005;24:887–897. doi: 10.1016/j.neuroimage.2004.09.026. [DOI] [PubMed] [Google Scholar]
- 41.Waldemann MR, Dieterich JH. Throwing a bomb on a person versus throwing a person on a bomb: intervention myopia in moral intuitions. Psychol Sci. 2007;18:247–253. doi: 10.1111/j.1467-9280.2007.01884.x. [DOI] [PubMed] [Google Scholar]
- 42.Young L, Saxe R. An fMRI investigation of Spontaneous Mental State Inference for Moral judgment. J Cogn Neurosci. 2009;21:1396–1405. doi: 10.1162/jocn.2009.21137. [DOI] [PubMed] [Google Scholar]
- 43.Zahn R, Moll J, Iyengar V, et al. Social conceptual impairments in frontotemporal lobar degeneration with right anterior temporal hypometabolism. Brain. 2009;132:604–616. doi: 10.1093/brain/awn343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Takahashi H, Kato M, Matsuura M, et al. Neural correlates of human virtue judgment. Cerebral Cortex. 2008;18:1886–1891. doi: 10.1093/cercor/bhm214. [DOI] [PubMed] [Google Scholar]
- 45.Greene J, Haidt J. How (and where) does moral judgment work? Trends Cogn Sci. 2002;6:517–523. doi: 10.1016/s1364-6613(02)02011-9. [DOI] [PubMed] [Google Scholar]
- 46.Greene J. From neural ‘is’ to moral ‘ought’: what are the moral implications of neuroscientific moral psychology? Nat Rev Neurosci. 2003;4:846–849. doi: 10.1038/nrn1224. [DOI] [PubMed] [Google Scholar]
- 47.Greene JD. Why are VMPFC patients more utilitarian? A dual-process theory of moral judgment explains. Trends Cogn Sci. 2007;11:322–323. doi: 10.1016/j.tics.2007.06.004. [DOI] [PubMed] [Google Scholar]
- 48.Nichols S, Mallon R. Moral dilemmas and moral rules. Cognition. 2006;100:530–542. doi: 10.1016/j.cognition.2005.07.005. [DOI] [PubMed] [Google Scholar]
- 49.Prehn K, Wartenberger I, Mériau K, et al. Individual differences in moral judgment competence influence neural correlates of socio-normative judgments. Soc Cogn Affect Neurosci. 2008;2:33–46. doi: 10.1093/scan/nsm037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Miller G. Neurobiology. The roots of morality. Science. 2008;320:734–737. doi: 10.1126/science.320.5877.734. [DOI] [PubMed] [Google Scholar]
- 51.De Quervain DJ-F, Fischbacher U, Treyer V, et al. The neural basis of altruistic punishment. Science. 2004;305:1254–1258. doi: 10.1126/science.1100735. [DOI] [PubMed] [Google Scholar]
- 52.Tabibnia G, Satpute AB, Lieberman MD. The sunny side of fairness: preference for fairness activates reward circuitry (and disregarding unfairness activates self-control circuitry) Psychol Sci. 2008;19:339–347. doi: 10.1111/j.1467-9280.2008.02091.x. [DOI] [PubMed] [Google Scholar]
- 53.Talmi D, Frith C. Neurobiology–feeling right about doing right. Nature. 2007;446:865–866. doi: 10.1038/446865a. [DOI] [PubMed] [Google Scholar]
- 54.Kliemann D, Young L, Scholz J, Saxe R. The influence of prior record on moral judgment. Neuropsychologia. 2008;46:2949–2957. doi: 10.1016/j.neuropsychologia.2008.06.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Amodio DM, Frith CD. Meeting of minds: the medial frontal cortex and social cognition. Nat Rev Neurosci. 2006;7:268–277. doi: 10.1038/nrn1884. [DOI] [PubMed] [Google Scholar]
- 56.Knoch D, Nitsche MA, Fischbacher U, Eisenegger C, Pascual-Leone A, Fehr E. Studying the neurobiology of social interaction with transcranial direct current stimulation-- the example of punishing unfairness. Cereb Cortex. 2008;18:1987–1990. doi: 10.1093/cercor/bhm237. [DOI] [PubMed] [Google Scholar]
- 57.Bechara A, Damasio H, Damasio AR. Emotion, decision making and the orbitofrontal cortex. Cereb Cortex. 2000;10:295–307. doi: 10.1093/cercor/10.3.295. [DOI] [PubMed] [Google Scholar]
- 58.Zahn R, Moll J, Paiva M, et al. The neural basis of human social values: evidence from functional MRI. Cerebr Cortex. 2009;19:276–283. doi: 10.1093/cercor/bhn080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Blair RJR. The roles of orbital frontal cortex in the modulation of antisocial behavior. Brain Cogn. 2004;55:198–208. doi: 10.1016/S0278-2626(03)00276-8. [DOI] [PubMed] [Google Scholar]
- 60.Blair J, Mitchell D, Blair K. The Psychopath. Emotion and the Brain. Oxford, England: Blackwell Publishing; 2005. [Google Scholar]
- 61.Blair RJ. Applying a cognitive neuroscience perspective to the disorder of psychopathy. Dev Psychopathol. 2005;17:865–891. doi: 10.1017/S0954579405050418. [DOI] [PubMed] [Google Scholar]
- 62.Bird CM, Castelli F, Malik O, Frith U, Husain M. The impact of extensive medial frontal lobe damage on ‘Theory of Mind’ and cognition. Brain. 2004;127:914–928. doi: 10.1093/brain/awh108. [DOI] [PubMed] [Google Scholar]
- 63.Berthoz S, Armony JL, Blair RJ, Dolan RJ. An fMRI study of intentional and unintentional (embarrassing) violations of social norms. Brain. 2002;125:1696–1708. doi: 10.1093/brain/awf190. [DOI] [PubMed] [Google Scholar]
- 64.De Waal FB. Putting the altruism back into altruism: the evolution of empathy. Annu Rev Psychol. 2007;59:1–22. doi: 10.1146/annurev.psych.59.103006.093625. [DOI] [PubMed] [Google Scholar]
- 65.Shamay-Tsoory SG, Aharon-Peretz J, Perry D. Two systems for empathy: a double dissociation between emotional and cognitive empathy in inferior frontal gyrus versus ventromedial prefrontal lesions. Brain. 2009;132:617–627. doi: 10.1093/brain/awn279. [DOI] [PubMed] [Google Scholar]
- 66.Eslinger PJ. Neurological and neuropsychological bases of empathy. Eur Neurol. 1998;39:193–199. doi: 10.1159/000007933. [DOI] [PubMed] [Google Scholar]
- 67.Gallese V. Before and below ‘theory of mind’: embodied simulation and the neural correlates of social cognition. Philos Trans R Soc Lond B Biol Sci. 2007;362:659–669. doi: 10.1098/rstb.2006.2002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Shamay-Tsoory SG, Tomer R, Berger BD, Aharon-Peretz J. Characterization of empathy deficits following prefrontal brain damage: the role of the right ventromedial prefrontal cortex. J Cogn Neurosci. 2003;15:324–337. doi: 10.1162/089892903321593063. [DOI] [PubMed] [Google Scholar]
- 69.Singer T. The neuronal basis and ontogeny of empathy and mind reading: review of literature and implications for future research. Neurosci Biobehav Rev. 2006;30:855–863. doi: 10.1016/j.neubiorev.2006.06.011. [DOI] [PubMed] [Google Scholar]
- 70.Carr L, Iacoboni M, Dubeau M-C, Mazziotta JC, Lenzi JL. Neural mechanisms of empathy in humans: a relay from neural systems for imitation to limbic areas. Proc Natl Acad Sci USA. 2003;100:5497–5502. doi: 10.1073/pnas.0935845100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Nummenmaa L, Hirvonen J, Parkkola R, Hietanen JK. Is emotional contagion special? An fMRI study on neural systems for affective and cognitive empathy. Neuroimage. 2008;43:571–580. doi: 10.1016/j.neuroimage.2008.08.014. [DOI] [PubMed] [Google Scholar]
- 72.Mitchell JP, Banaji MR, Macrae CN. The link between social cognition and self-referential thought in the medial prefrontal cortex. J Cogn Neurosci. 2005;17:1306–1315. doi: 10.1162/0898929055002418. [DOI] [PubMed] [Google Scholar]
- 73.Iacoboni M, Mazziotta JC. Mirror neuron system: basic findings and clinical applications. Ann Neurol. 2007;62:213–218. doi: 10.1002/ana.21198. [DOI] [PubMed] [Google Scholar]
- 74.Rizzolatti G, Fabbri-Destro M. The mirror system and its role in social cognition. Curr Opin Neurobiol. 2008;18:179–184. doi: 10.1016/j.conb.2008.08.001. [DOI] [PubMed] [Google Scholar]
- 75.Oberman LM, Pineda JA, Ramachandran VS. The human mirror neuron system: A link between action observation and social skills. Soc Cogn Affect Neurosci. 2007;2:62–66. doi: 10.1093/scan/nsl022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Preston SD, de Waal FB. Empathy: Its ultimate and proximate bases. Behav Brain Sci. 2002;25:1–20. doi: 10.1017/s0140525x02000018. [DOI] [PubMed] [Google Scholar]
- 77.Schulte-Ruther M, Markowitsch HJ, Fink GR, Piefke M. Mirror neuron and theory of mind mechanisms involved in face-to-face interactions: a functional magnetic resonance imaging approach to empathy. J Cogn Neurosci. 2007;19:1354–1372. doi: 10.1162/jocn.2007.19.8.1354. [DOI] [PubMed] [Google Scholar]
- 78.Kaplan JT, Iacoboni M. Getting a grip on other minds: mirror neurons, intention understanding, and cognitive empathy. Soc Neurosci. 2006;1:175–183. doi: 10.1080/17470910600985605. [DOI] [PubMed] [Google Scholar]
- 79.Kédia G, Berthoz S, Wessa M, Hilton D, Martinot JL. An agent harms a victim: a functional magnetic resonance imaging study on specific moral emotions. Cogn Neurosci. 2008;20:1788–1798. doi: 10.1162/jocn.2008.20070. [DOI] [PubMed] [Google Scholar]
- 80.Lamm C, Batson CD, Decety J. The neural substrate of human empathy: effects of perspective-taking and cognitive appraisal. J Cogn Neurosci. 2007;19:42–58. doi: 10.1162/jocn.2007.19.1.42. [DOI] [PubMed] [Google Scholar]
- 81.Lieberman MD. Social cognitive neuroscience: a review of core processes. Ann Rev Psychol. 2007;58:259–289. doi: 10.1146/annurev.psych.58.110405.085654. [DOI] [PubMed] [Google Scholar]
- 82.Schilbach L, Wohlschlaeger AM, Kraemer NC, et al. Being with virtual others: neurological correlates of social interaction. Neuropsychologia. 2006;44:718–730. doi: 10.1016/j.neuropsychologia.2005.07.017. [DOI] [PubMed] [Google Scholar]
- 83.Markowitsch HJ. Neuroscience and crime. Neurocase. 2008;14:1–6. doi: 10.1080/13554790801994756. [DOI] [PubMed] [Google Scholar]
- 84.Intrator J, Hare R, Stritzke P, et al. A brain imaging (single photon emission computerized tomography) study of semantic and affective processing in psychopaths. Biol Psychiatry. 1997;42:96–103. doi: 10.1016/S0006-3223(96)00290-9. [DOI] [PubMed] [Google Scholar]
- 85.Levenston GK, Patrick CJ, Bradley MM, Lang PJ. The psychopath as observer: emotion and attention in picture processing. J Abnorm Psychol. 2000;109:373–385. [PubMed] [Google Scholar]
- 86.Raine A, Buchsbaum M, LaCasse L. Brain abnormalities in murderers indicated by positron emission tomography. Biol Psychiatry. 1997;42:495–508. doi: 10.1016/S0006-3223(96)00362-9. [DOI] [PubMed] [Google Scholar]
- 87.Blake PY, Pincus JH, Buckner C. Neurologic abnormalities in murderers. Neurology. 1995;45:1641–1647. doi: 10.1212/wnl.45.9.1641. [DOI] [PubMed] [Google Scholar]
- 88.Wong MT, Lumsden J, Fenton GW, Fenwick PB. Electroencephalography, computed tomography and violence ratings of male patients in a maximum-security mental hospital. Acta Psychiatr Scand. 1994;90:97–101. doi: 10.1111/j.1600-0447.1994.tb01562.x. [DOI] [PubMed] [Google Scholar]
- 89.Critchley HD, Simmons A, Daly EM, et al. Prefrontal and medial temporal correlates of repetitive violence to self and others. Biol Psychiatry. 2000;47:928–934. doi: 10.1016/s0006-3223(00)00231-6. [DOI] [PubMed] [Google Scholar]
- 90.Ishikawa SS, Raine A, Lencz T, Bihrle S, Lacasse L. Autonomic stress reactivity and executive functions in successful and unsuccessful criminal psychopaths from the community. J Abnorm Psychol. 2001;110:423–432. doi: 10.1037//0021-843x.110.3.423. [DOI] [PubMed] [Google Scholar]
- 91.Krakowski M, Czobor P, Carpenter MD, et al. Community violence and inpatient assaults: neurobiological deficits. J Neuropsychiatry Clin Neurosci. 1997;9:549–555. doi: 10.1176/jnp.9.4.549. [DOI] [PubMed] [Google Scholar]
- 92.LaPierre D, Braun CMJ, Hodgins S. Ventral frontal deficits in psychopathy: neuropsychological test findings. Neuropsychologia. 1995;33:139–151. doi: 10.1016/0028-3932(94)00110-b. [DOI] [PubMed] [Google Scholar]
- 93.Moffitt TE. Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy. Psychol Rev. 1993;100:674–701. [PubMed] [Google Scholar]
- 94.Raine A, Meloy JR, Bihrle S, Stoddard J, LaCasse L, Buchsbaum MS. Reduced prefrontal and increased subcortical brain functioning assessed using positron emission tomography in predatory and affective murderers. Behav Sci Law. 1998;16:319–332. doi: 10.1002/(sici)1099-0798(199822)16:3<319::aid-bsl311>3.0.co;2-g. [DOI] [PubMed] [Google Scholar]
- 95.Seidenwurm D, Pounds TR, Globus A, Valk PE. Abnormal temporal lobe metabolism in violent subjects: correlation of imaging and neuropsychiatric findings. Am J Neuroradiol. 1997;18:625–631. [PMC free article] [PubMed] [Google Scholar]
- 96.Soderstrom H, Hultin L, Tullberg M, Wikkelso C, Ekholm S, Forsman A. Reduced frontotemporal perfusion in psychopathic personality. Psychiatry Res. 2002;114:81–94. doi: 10.1016/s0925-4927(02)00006-9. [DOI] [PubMed] [Google Scholar]
- 97.Hoptman MJ. Neuroimaging studies of violence and antisocial behavior. J Psychiatr Pract. 2003;9:265–278. doi: 10.1097/00131746-200307000-00002. [DOI] [PubMed] [Google Scholar]
- 98.De Oliveira-Souza R, Hare RD, Bramati IE, et al. Psychopathy as a disorder of the moral brain: fronto-temporo-limbic grey matter reductions demonstrated by voxel-based morphometry. Neuroimage. 2008;40:1202–1213. doi: 10.1016/j.neuroimage.2007.12.054. [DOI] [PubMed] [Google Scholar]
- 99.Tiihonen J, Rossi R, Laakso MP, et al. Brain anatomy of persistent violent offenders: more rather than less. Psychiatry Res. 2008;163:201–212. doi: 10.1016/j.pscychresns.2007.08.012. [DOI] [PubMed] [Google Scholar]
- 100.Raine A, Lencz T, Bihrle S, LaCasse L, Colletti P. Reduced prefrontal gray matter volume and reduced autonomic activity in antisocial personality disorder. Arch Gen Psychiatry. 2000;57:119–127. doi: 10.1001/archpsyc.57.2.119. [DOI] [PubMed] [Google Scholar]
- 101.Sapolsky RM. The frontal cortex and the criminal justice system. Philos Trans R Soc Lond B Biol Sci. 2004;359:1787–1796. doi: 10.1098/rstb.2004.1547. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.De Brito SA, Mechelli A, Wilke M, et al. Size matters: Increased grey matter in boys with conduct problems and callous-unemotional traits. Brain. 2009;132:843–852. doi: 10.1093/brain/awp011. [DOI] [PubMed] [Google Scholar]
- 103.Veit R, Flor H, Erb M, et al. Brain circuits involved in emotional learning in antisocial behavior and social phobia in humans. Neurosci Lett. 2002;328:233–236. doi: 10.1016/s0304-3940(02)00519-0. [DOI] [PubMed] [Google Scholar]
- 104.Finger EC, Marsh AA, Mitchell DG, et al. Abnormal ventromedial prefrontal cortex function in children with psychopathic traits during reversal learning. Arch Gen Psychiatry. 2008;65:586–594. doi: 10.1001/archpsyc.65.5.586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 105.Blair RJ. The amygdala and ventromedial prefrontal cortex in morality and psychopathy. Trends Cogn Sci. 2007;11:387–392. doi: 10.1016/j.tics.2007.07.003. [DOI] [PubMed] [Google Scholar]
- 106.Cohen L, Angladette L, Benoit N, Pierrot-Deseilligny C. A man who borrowed cars. Lancet. 1999;353:34. doi: 10.1016/S0140-6736(98)09047-3. [DOI] [PubMed] [Google Scholar]
- 107.Paradiso S, Robinson RG, Arndt S. Self-reported aggressive behavior in patients with stroke. J Nerv Ment Dis. 1996;184:746–753. doi: 10.1097/00005053-199612000-00005. [DOI] [PubMed] [Google Scholar]
- 108.Pillmann F, Rohde A, Ullrich S, Draba S, Sannemüller U, Marneros A. Violence, criminal behavior, and the EEG: significance of left hemispheric focal abnormalities. J Neuropsychiatry Clin Neurosci. 1999;11:454–457. doi: 10.1176/jnp.11.4.454. [DOI] [PubMed] [Google Scholar]
- 109.Anderson SW, Bechara A, Damasio H, Tranel D, Damasio AR. Impairment of social and moral behavior related to early damage in human prefrontal cortex. Nat Neurosci. 1999;2:1031–1037. doi: 10.1038/14833. [DOI] [PubMed] [Google Scholar]
- 110.Eslinger PJ, Flaherty-Craig CV, Benton AL. Developmental outcomes after early prefrontal cortex damage. Brain Cogn. 2004;55:84–103. doi: 10.1016/S0278-2626(03)00281-1. [DOI] [PubMed] [Google Scholar]
- 111.Bechara A, Tranel D, Damasio H. Characterization of the decision-making deficit of patients with ventromedial prefrontal cortex lesions. Brain. 2000;123:2189–2202. doi: 10.1093/brain/123.11.2189. [DOI] [PubMed] [Google Scholar]
- 112.Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition. 1994;50:7–15. doi: 10.1016/0010-0277(94)90018-3. [DOI] [PubMed] [Google Scholar]
- 113.Blair RJR, Cipolotti L. Impaired social response reversal. A case of ‘acquired sociopathy’. Brain. 2000;123:1122–1141. doi: 10.1093/brain/123.6.1122. [DOI] [PubMed] [Google Scholar]
- 114.Ciaramelli E, Muccioli M, Ladavas E, di Pellegrino G. Selective deficit in personal moral judgment following damage to ventromedial prefrontal cortex. Soc Cogn Affect Neurosci. 2007;2:84–92. doi: 10.1093/scan/nsm001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Cushman FA, Young LL, Hauser MD. The role of conscious reasoning and intuition in moral judgments: Testing three principles of permissible harm. Psychol Sci. 2006;17:1082–1089. doi: 10.1111/j.1467-9280.2006.01834.x. [DOI] [PubMed] [Google Scholar]
- 116.Damasio AR, Tranel D, Damasio H. Individuals with sociopathic behavior caused by frontal damage fail to respond autonomically to social stimuli. Behav Brain Res. 1990;41:81–94. doi: 10.1016/0166-4328(90)90144-4. [DOI] [PubMed] [Google Scholar]
- 117.Koenigs M, Young L, Adolphs R, Tranel D, Cushman F, Hauser M, Damasio A. Damage to the prefrontal cortex increases utilitarian moral judgments. Nature. 2007;446:908–911. doi: 10.1038/nature05631. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 118.Shamay-Tsoory SG, Tomer R, Berger BD, Goldsher D, Aharon-Peretz J. Impaired “affective theory of mind” is associated with right ventromedial prefrontal damage. Cogn Behav Neurol. 2005;18:55–67. doi: 10.1097/01.wnn.0000152228.90129.99. [DOI] [PubMed] [Google Scholar]
- 119.Tranel D, Bechara A, Denburg NL. Asymmetric functional roles of right and left ventromedial prefrontal cortices in social conduct, decision-making, and emotional processing. Cortex. 2002;38:589–612. doi: 10.1016/s0010-9452(08)70024-8. [DOI] [PubMed] [Google Scholar]
- 120.Tranel D. “Acquired sociopathy”: the development of sociopathic behavior following focal brain damage. Prog Exp Pers Psychopathol Res. 1994:285–311. [PubMed] [Google Scholar]
- 121.Beer JS, Heerey EA, Keltner D, Scabini D, Knight RT. The regulatory function of self-conscious emotion: Insights from patients with orbitofrontal damage. J Pers Soc Psychol. 2003;85:594–604. doi: 10.1037/0022-3514.85.4.594. [DOI] [PubMed] [Google Scholar]
- 122.Beer JS, John OP, Scabini D, Knight RT. Orbitofrontal cortex and social behavior: integrating self-monitoring and emotion-cognition interactions. J Cong Neurosci. 2006;18:871–879. doi: 10.1162/jocn.2006.18.6.871. [DOI] [PubMed] [Google Scholar]
- 123.Eslinger PJ, Grattan LM, Damasio AF. Developmental consequences of childhood frontal lobe damage. Arch Neurol. 1992;49:764–769. doi: 10.1001/archneur.1992.00530310112021. [DOI] [PubMed] [Google Scholar]
- 124.Shamay-Tsoory SG, Tibi-Elhanany Y, Aharon-Peretz J. The green-eyed monster and malicious joy: the neuroanatomical bases of envy and gloating (schadenfreude) Brain. 2007;130:1663–1678. doi: 10.1093/brain/awm093. [DOI] [PubMed] [Google Scholar]
- 125.Lough S, Hodges JR. Measuring and modifying abnormal social cognition in frontal variant frontotemporal dementia. J Psychosom Res. 2002;53:639–646. doi: 10.1016/s0022-3999(02)00433-6. [DOI] [PubMed] [Google Scholar]
- 126.Scarpa A, Raine A. Psychophysiology of anger and violent behavior. Psychiatr Clin North Am. 1997;20:375–394. doi: 10.1016/s0193-953x(05)70318-x. [DOI] [PubMed] [Google Scholar]
- 127.Zlotnick C. Antisocial personality disorder, affect dysregulation and childhood abuse among incarcerated women. J Personal Disord. 1999;13:90–95. doi: 10.1521/pedi.1999.13.1.90. [DOI] [PubMed] [Google Scholar]
- 128.Brower MC, Price BH. Neuropsychiatry of frontal lobe dysfunction in violent and criminal behaviour: a critical review. J Neurol Neurosurg Psychiatry. 2001;71:720–726. doi: 10.1136/jnnp.71.6.720. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 129.Koenigs M, Tranel D. Irrational economic decision-making after ventromedial prefrontal damage: evidence from the ultimatum game. J Neurosci. 2007;21:951–956. doi: 10.1523/JNEUROSCI.4606-06.2007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 130.Anderson SW, Barrash J, Bechara A, Tranel D. Impairments of emotion and realword complex behavior following childhood- or adult-onset damage to ventromedial prefrontal cortex. J Int Neuropsychol Soc. 2006;12:224–235. doi: 10.1017/S1355617706060346. [DOI] [PubMed] [Google Scholar]
- 131.Burgess PW, Alderman N, Forbes C, et al. The case for the development and use of “ecologically valid” measures of executive functions in experimental and clinical neuropsychology. J Int Neuropsychol Soc. 2006;12:194–209. doi: 10.1017/S1355617706060310. [DOI] [PubMed] [Google Scholar]
- 132.Saver JL, Damasio AR. Preserved access and processing of social knowledge in a patient with acquired sociopathy due to ventromedial frontal damage. Neuropsychologia. 1991;29:1241–1249. doi: 10.1016/0028-3932(91)90037-9. [DOI] [PubMed] [Google Scholar]
- 133.Barrash J, Tranel D, Anderson SW. Acquired personality disturbances associated with bilateral damage to the ventromedial prefrontal region. Develop Neuropsychol. 2000;18:355–381. doi: 10.1207/S1532694205Barrash. [DOI] [PubMed] [Google Scholar]
- 134.Bechara A, Van Der Linden M. Decision-making and impulse control after frontal lobe injuries. Curr Opin Neurol. 2005;18:734–739. doi: 10.1097/01.wco.0000194141.56429.3c. [DOI] [PubMed] [Google Scholar]
- 135.Camille N, Coricelli G, Sallet J, Pradat-Diehl P, Duhamel JR, Sirigu A. The involvement of the orbitofrontal cortex in the experience of regret. Science. 2004;304:1167–1170. doi: 10.1126/science.1094550. [DOI] [PubMed] [Google Scholar]
- 136.Lough S, Kipps CM, Treise C, Watson P, Blair JR, Hodges JR. Social reasoning, emotion and empathy in frontotemporal dementia. Neuropsychologia. 2006;44:950–958. doi: 10.1016/j.neuropsychologia.2005.08.009. [DOI] [PubMed] [Google Scholar]
- 137.Mah LW, Arnold MC, Grafman J. Deficits in social knowledge following damage to ventromedial prefrontal cortex. J Neuropsychiatry Clin Neurosci. 2005;17:66–74. doi: 10.1176/jnp.17.1.66. [DOI] [PubMed] [Google Scholar]
- 138.Neary D, Snowden J, Gustafson L, et al. Frontotemporal lobar degeneration: a consensus on clinical diagnostic criteria. Neurology. 1998;51:1546–1552. doi: 10.1212/wnl.51.6.1546. [DOI] [PubMed] [Google Scholar]
- 139.Miller BL, Chang L, Mena I, Boone K, Lesser IM. Progressive right frontotemporal degeneration: clinical, neuropsychological and SPECT characteristics. Dementia. 1993;4:204–213. doi: 10.1159/000107324. [DOI] [PubMed] [Google Scholar]
- 140.Edwards-Lee T, Miller BL, Benson DF, et al. The temporal variant of frontotemporal dementia. Brain. 1997;120:1027–1040. doi: 10.1093/brain/120.6.1027. [DOI] [PubMed] [Google Scholar]
- 141.Mychack P, Kramer JH, Boone KB, Miller BL. The influence of right frontotemporal dysfunction on social behavior in frontotemporal dementia. Neurology. 2001;56(Suppl 4):S11–S15. doi: 10.1212/wnl.56.suppl_4.s11. [DOI] [PubMed] [Google Scholar]
- 142.Perry RJ, Rosen HR, Kramer JH, Beer JS, Levenson RL, Miller BL. Hemispheric dominance for emotions, empathy and social behaviour: Evidence from right and left handers with frontotemporal dementia. Neurocase. 2001;7:145–160. doi: 10.1093/neucas/7.2.145. [DOI] [PubMed] [Google Scholar]
- 143.Mendez MF, Lim GTH. Alterations in the sense of ‘humanness’ in right hemisphere predominant FTD patients. Cogn Behav Neurol. 2004;17:133–138. doi: 10.1097/01.wnn.0000136593.21532.16. [DOI] [PubMed] [Google Scholar]
- 144.Mendez MF, Lauterbach E, Sampson S ANPA Committee on Research. An Evidence- Based Review of the Psychopathology of Frontotemporal Dementia: A Report of the ANPA Committee on Research. J Neuropsychiatry Clin Neurosci. 2008;20:130–149. doi: 10.1176/jnp.2008.20.2.130. [DOI] [PubMed] [Google Scholar]
- 145.Mendez MF, Chen AK, Shapira JS, Miller BL. Acquired sociopathy and frontotemporal dementia. Dement Geriatr Cogn Disord. 2005;20:99–104. doi: 10.1159/000086474. [DOI] [PubMed] [Google Scholar]
- 146.Gustafson L. Clinical picture of frontal lobe degeneration of non-Alzheimer type. Dementia. 1993;4:143–148. doi: 10.1159/000107313. [DOI] [PubMed] [Google Scholar]
- 147.Lynch T, Sano M, Marder KS, et al. Clinical characteristics of a family with chromosome 17-linked disinhibition-dementia-parkinsonism-amyotrophy complex. Neurology. 1994;44:1878–1884. doi: 10.1212/wnl.44.10.1878. [DOI] [PubMed] [Google Scholar]
- 148.Miller BL, Darby A, Benson DF, Cummings JL, Miller MH. Aggressive, socially disruptive and antisocial behaviour associated with fronto-temporal dementia. Br J Psychiatry. 1997;170:150–154. doi: 10.1192/bjp.170.2.150. [DOI] [PubMed] [Google Scholar]
- 149.Mendez MF, Chow T, Ringman J, Twitchell G, Hinkin CH. Pedophilia and disturbances of the temporal lobes. J Neuropsychiatry Clin Neurosci. 2000;12:71–76. doi: 10.1176/jnp.12.1.71. [DOI] [PubMed] [Google Scholar]
- 150.Mendez MF, Anderson E, Shapira JS. An investigation of moral judgment in frontotemporal dementia. Cogn Behav Neurol. 2005;18:193–197. doi: 10.1097/01.wnn.0000191292.17964.bb. [DOI] [PubMed] [Google Scholar]
- 151.Rankin KP, Kramer JH, Miller BL. Patterns of cognitive and emotional empathy in frontotemporal lobar degeneration. Cogn Behav Neurol. 2005;18:28–36. doi: 10.1097/01.wnn.0000152225.05377.ab. [DOI] [PubMed] [Google Scholar]
- 152.Rankin KP, Kramer JH, Mychack P, Miller BL. Double dissociation of social functioning in frontotemporal dementia. Neurology. 2003;60:266–271. doi: 10.1212/01.wnl.0000041497.07694.d2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 153.Rankin KP, Rosen HJ, Kramer JH, et al. Right and left medial orbitofrontal volumes show an opposite relationship to agreeableness in FTD. Dement Geriatr Cogn Disord. 2004;17:328–332. doi: 10.1159/000077165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 154.Gorno-Tempini ML, Rankin KP, Woolley JD, Rosen HJ, Phengrasamy L, Miller BL. Cognitive and behavioral profile in a case of right anterior temporal lobe neurodegeneration. Cortex. 2004;40:631–644. doi: 10.1016/s0010-9452(08)70159-x. [DOI] [PubMed] [Google Scholar]
- 155.Rankin KP, Gorno-Tempini ML, Allison SC, et al. Structural anatomy of empathy in neurodegenerative disease. Brain. 2006;129:2945–2956. doi: 10.1093/brain/awl254. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 156.Snowden JS, Gibbons ZC, Blackshaw A, et al. Social cognition in frontotemporal dementia and Huntington’s disease. Neuropsychologia. 2003;41:688–701. doi: 10.1016/s0028-3932(02)00221-x. [DOI] [PubMed] [Google Scholar]
- 157.Gregory C, Lough S, Stone V, et al. Theory of mind in patients with frontal variant frontotemporal dementia and Alzheimer’s disease: theoretical and practical implications. Brain. 2002;125:752–764. doi: 10.1093/brain/awf079. [DOI] [PubMed] [Google Scholar]
- 158.Lough S, Gregory C, Hodges JR. Dissociation of social cognition and executive function in frontal variant frontotemporal dementia. Neurocase. 2001;7:123–130. doi: 10.1093/neucas/7.2.123. [DOI] [PubMed] [Google Scholar]
- 159.Hauser MD. The liver and the moral organ. Soc Cogn Affect Neurosci. 2006;1:214–220. doi: 10.1093/scan/nsl026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 160.Mikhail J. Universal moral grammar: theory, evidence and the future. Trends Cogn Sci. 2007;11:143–152. doi: 10.1016/j.tics.2006.12.007. [DOI] [PubMed] [Google Scholar]
- 161.Pijnenburg YA. The roots of social inappropriateness in frontotemporal dementia. J Neurol Neurosurg Psychiatry. 2007;78:441. doi: 10.1136/jnnp.2006.107805. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 162.Moll J, de Oliveira-Souza R, Garrido GJ, et al. The self as a moral agent: linking the neural bases of social agency and moral sensitivity. Soc Neurosci. 2007;2:336–352. doi: 10.1080/17470910701392024. [DOI] [PubMed] [Google Scholar]
- 163.Shallice T. ‘Theory of mind’ and the prefrontal cortex. Brain. 2001;124:247–248. doi: 10.1093/brain/124.2.247. [DOI] [PubMed] [Google Scholar]
- 164.Stone VE, Baron-Cohen S, Calder A, Keane J, Young A. Acquired theory of mind impairments in individuals with bilateral amygdalar lesions. Neuropsychologia. 2003;41:209–220. doi: 10.1016/s0028-3932(02)00151-3. [DOI] [PubMed] [Google Scholar]
- 165.Stuss DT, Gallup GG, Jr, Alexander MP. The frontal lobes are necessary for theory of mind. Brain. 2001;124:279–286. doi: 10.1093/brain/124.2.279. [DOI] [PubMed] [Google Scholar]
- 166.Tankersley D, Stowe CJ, Huettel SA. Altruism is associated with an increased neural response to agency. Nat Neurosci. 2007;10:150–151. doi: 10.1038/nn1833. [DOI] [PubMed] [Google Scholar]
- 167.Calarge C, Andreasen NC, O’Leary DS. Visualizing how one brain understands another: a PET study of theory of mind. Am J Psychiatry. 2003;160:1954–1964. doi: 10.1176/appi.ajp.160.11.1954. [DOI] [PubMed] [Google Scholar]
- 168.Borum R, Fulero SM. Empirical research on the insanity defense and attempted reforms: evidence toward informed policy. Law Hum Behav. 1999;23:375–393. doi: 10.1023/a:1022364700424. [DOI] [PubMed] [Google Scholar]
- 169.Goodenough OR, Prehn K. A neuroscientific approach to normative judgment in law and justice. Philos Trans R Soc Lond B Biol Sci. 2004;359:1709–1726. doi: 10.1098/rstb.2004.1552. [DOI] [PMC free article] [PubMed] [Google Scholar]