
Fig. 1.
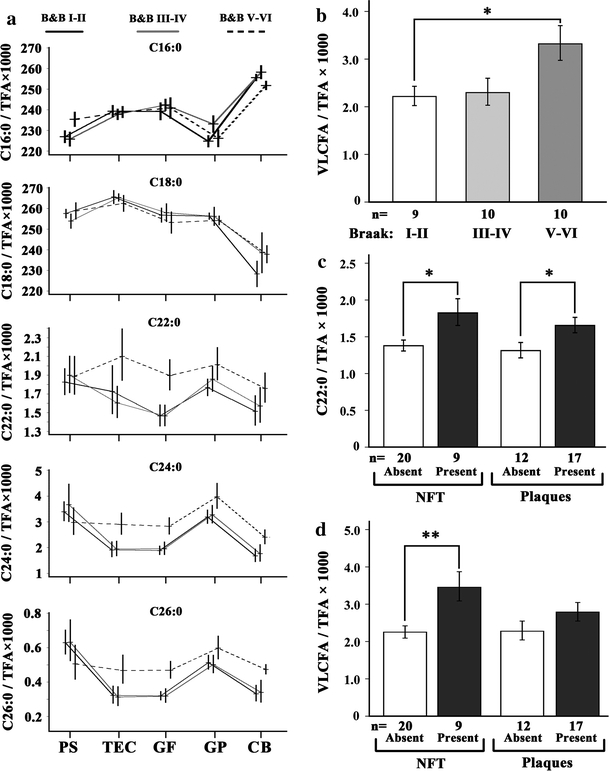
Accumulation of VLCFA in cortical areas of human brains associated with progressive AD neuropathology. a The content of long and very long-chain fatty acids in five different cortical regions, indicated below the graphs, was determined by GC–MS (n = 10/group). Relative amounts of the fatty acids C16:0, C18:0, C22:0, C24:0 and C26:0 are depicted as ratio to the total fatty acid (TFA) content (×1,000). The mean values of each AD severity group are connected across brain regions by the line pattern indicated above the graphs. The AD-related neuropathology was defined according to Braak staging of the contralateral hemisphere. Tissue abbreviations: PS parasubiculum, TEC trans-entorhinal cortex, GF gyrus frontalis, GP gyrus precentralis, CB cerebellar cortex. The mean level of VLCFA (C24:0 and C26:0 combined) in gyrus frontalis is depicted as ratio to total fatty acids for the three Braak stage groups (b) and of C22:0 (c) and VLCFA (d) in relation to NFT and plaques. The increase in VLCFA in stage V–VI when compared with stage I–II was statistically significant (corr. p = 0.044). When NFT were present, both C22:0 (c left) and VLCFA (d left) were significantly increased (p = 0.013 and 0.003, respectively). Also when the cases were grouped according to plaques, the levels of C22:0 (c right) and VLCFA (d right) were elevated when plaques were present, but to a lesser extent (p = 0.030 and 0.165, respectively). Thus, the increase in VLCFA was more strongly associated with NFT than with plaques. Error bars indicate SEM; *p < 0.05 and **p < 0.01; corr., corrected for multiple testing (Tukey’s post hoc test)