

Abstract
Objectives: To examine the types of questions received by Clinical Informatics Consult Service (CICS) librarians from clinicians on rounds and to analyze the number of clearly differentiated viewpoints provided in response.
Design: Questions were retrieved from an internal database, the CICS Knowledge Base, and analyzed for redundancy by subject analysis. The unique questions were classified into ten categories by subject. Treatment-related questions were analyzed for the number of viewpoints represented in the librarian's response.
Results: The CICS Knowledge Base contained 476 unique questions and 71 redundant questions. Among the unique queries, the top two categories accounted for 67%: treatment (36%) and disease description (31%). Within the treatment-related subset, 138 questions (59%) required representation of more than one viewpoint in the librarian's response.
Discussion: Questions generated by clinicians frequently require comprehensive, critical appraisal of the medical literature, a need that can be filled by librarians trained in such techniques. This study demonstrates that many questions require representation of more than one viewpoint to answer completely. Moreover, the redundancy rate underscores the need for resources like the CICS Knowledge Base. By critically analyzing the medical literature, CICS librarians are providing a time-saving and valuable service for clinicians and charting new territory for librarians.
INTRODUCTION
Discourses on the amount of medical information available and its exponential growth have become commonplace in the literature of information science and medicine. Patrick purports that complaints about the information explosion can even be found in the Bible [1]. In the often-cited, self-reporting study by Williamson et al., two-thirds of surveyed physicians note that the “current volume of scientific literature” is unmanageable [2]. Similarly, in a survey of 500 physicians, Hunt and Newman report that “when asked about time available for reading medical journals as compared with five years ago, a significant majority in each group of the respondents said less time was available for this activity” [3]. Indeed, MEDLINE alone contains more than eleven million citations, and more than 400,000 articles are added to the file each year [4]. Zipser notes that “to keep up with the 400,000 articles [added yearly], a physician could read two articles each day, every day of the year and by the end of the year fall 550 years behind” [5]. Similarly, Wyatt notes that the number of biomedical journals doubles approximately every nineteen years [6].
Given such astounding figures, coupled with the growing emphasis on evidence-based medicine (EBM) and its core tenet of “conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients” [7], it is no surprise that librarians are acting increasingly as intermediaries between clinicians and the vast amount of information available. Scherrer and Dorsch note that “EBM offers librarians the opportunity to participate fully in the information process” [8], while McKibbon remarks that “because clinicians who practice [evidence-based medicine] rely more on evidence found in the literature base than on clinical experience and pathophysiology alone, librarians play a key role in the advancement of” evidence-based medicine [9]. McKibbon further urges librarians to increase their knowledge of clinical study design and quality medical evidence, so that they can better assist physicians in the retrieval of information.
The Eskind Biomedical Library (EBL) at Vanderbilt University Medical Center (VUMC) has long subscribed to the idea that librarians are uniquely qualified to locate and evaluate medical information. Giuse has previously reported [10–12] on the EBL's innovative Clinical Informatics Consult Service (CICS), a program that expands the traditional idea of clinical medical librarianship (CML) [13–20]. The essential idea behind the CICS program is that librarians committed to “ongoing, lifelong expansion of skills and knowledge in medical specialty areas” can become truly integrated members of the clinical team who “analyze, interpret, and dissect complex medical searches to filter and summarize information to match the team's request appropriately” [21]. As described more fully by Giuse et al. [22], EBL's CICS program places librarians on rounds where they receive questions from any member of the clinical team, research those questions by extensively searching library resources, and select the most relevant, best evidentiary articles in answer to them. Rather than limiting their services simply to providing references as in traditional CML, CICS librarians filter the articles they select by reading, highlighting, and summarizing the articles as they relate to the clinical case at hand. Moreover, as Giuse notes, CICS librarians are careful to point out “conflicting data and opinions when a clear consensus is lacking” [23]. This type of service allows the librarians to meet the needs of clinicians most efficiently. Indeed, experience in working with clinicians on the CICS service as well as in the library itself has indicated that clinicians may not search for information with the same eye toward a comprehensive view of the available evidence. Clinicians generally prefer to locate a relatively small amount of highly relevant material in answer to a question.
This assumption is borne out in the types of resources to which clinicians generally turn for information: colleagues, who can likely provide a quick, relevant answer, and textbooks, which often provide concise synopses of thought on a topic. For instance, in their study of forty-nine physicians, Gorman and Helfand find that physicians rely most heavily on medical textbooks, clinical manuals, drug references, and other medical personnel as knowledge sources [24]. In a review of the literature regarding family physicians' use of information resources, Verhoeven et al. report that physicians most frequently consulted colleagues, books and journals, and libraries [25]. Haug, in a meta-analysis of twelve studies of physicians' resource use, has determined that physicians generally turn to books, journals, and colleagues to locate medical information. While not all of the studies included in Haug's analysis of physicians' use of resources differentiated between personal library and institutional library books and journals, it is reasonable to conclude that “physicians appeared to choose the sources of information that were most easily and efficiently accessed and most applicable to practical, clinical problems” [26]. Thus, clinicians, pressed for time and inundated by information, are not generally able to consider the multiple sources of evidence that an answer to a complex question may necessitate.
BACKGROUND
The ability of CICS librarians to examine diverse sources of evidence and interpret and synthesize medical articles is made possible by the librarians' understanding of clinical cases and their knowledgebase in the area in which they attend rounds. In addition to developing a knowledgebase in a medical specialty area, CICS librarians build expertise and confidence by participating in monthly training conferences that emphasize performing effective database searches, evaluating study design, weighing evidence provided by articles, and summarizing information properly. As discussed above, CICS librarians attempt to represent germane evidence from the literature by focusing on comprehensive information retrieval and hand filtering through their search results and articles to weigh and select the best evidence. Obviously, such critical appraisal of the medical evidence requires substantial time, a luxury not often available to the clinician. The CICS service is proving that properly trained librarians participating on rounds can act as Smith's hypothetical “ideal information source” that is “directly relevant, contain[s] valid information, and [is accessible] with a minimal amount of work” for clinicians [27].
Through an analysis of questions received by the CICS service, this paper will examine the program's continuing evolution toward acting as such a resource; the paper will illustrate how librarians, who “inhabit the intersection between a knowledge of information-seeking strategies and an understanding of the nuances of individual clinical cases,” are providing “a unique, value-added service which clinicians cannot necessarily duplicate on their own” [28]. Specifically, this paper reports a categorization of the kinds of questions received by CICS librarians on clinical rounds and an analysis of the numbers of clearly differentiated opinions or viewpoints represented in answers to those questions. The authors contend that by providing filtered information packets that represent and synthesize leading thought on complex questions, the CICS acts as a key evidence-based tool that allows the integration of “research evidence with the patient's clinical circumstances” [29] and can positively affect clinical decision making. Moreover, CICS allows librarians to assume new roles and effect the transformation into knowledge worker [30–32], a switch from information mediator to information synthesizer.
METHODS
Selection of clinical questions
CICS librarians entered all questions received on rounds and the type of requester, along with the references and summaries provided in response, into a MySQL relational database, the CICS Knowledge Base. A Perl common gateway interface (CGI) script provided a Web-based interface for question entry, search, and retrieval. All questions entered into this database between April 1, 1997, and November 30, 1999, were included in the initial analysis. We grouped the questions for analysis by clinical unit: Cardiac Intensive Care Unit (CICU), Hematology/Oncology Unit (Hem/Onc), Medical Intensive Care Unit (MICU), Neonatal Intensive Care Unit (NICU), Pediatric Intensive Care Unit (PICU), Surgical Intensive Care Unit (SICU), and Trauma Intensive Care Unit (Trauma).
Redundancy analysis
To calculate the number of questions occurring more than once, we identified redundant questions by a subject analysis of all CICS Knowledge Base records within each clinical unit. We selected the most recent record for each unique question for the purposes of the category and viewpoint examination; repeat occurrences were excluded from further analysis.
Category analysis
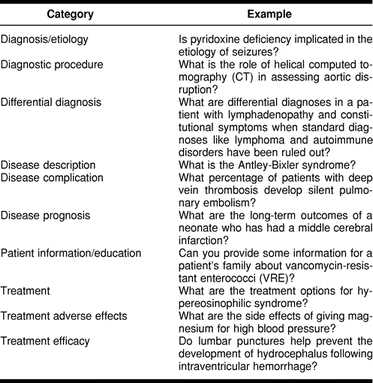
Each unique question was classified independently by the librarian on rounds and by another CICS librarian into one of ten categories (Table 1). These categories were adapted from those employed by Giuse et al. [33] and reviewed for clinical applicability for this study by two physicians. Librarians resolved disagreements in classification by discussion until consensus was reached.
Table 1 Categories and examples
Viewpoint analysis
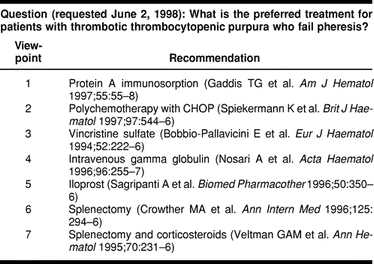
We defined a “viewpoint” as a clearly articulated opinion on or answer to a particular clinical question. Articles providing primary data were included in the analysis. Meta-analyses, systematic reviews, and practice guidelines were also included in this analysis as they provided an opinion based on a methodologically rigorous appraisal of the literature. Overview materials, such as general review articles, were excluded from the viewpoint analysis, because such items typically provide an overview of the existing thought on a topic rather than a true evidence-based opinion. Table 2 provides an example of a treatment-related question and the viewpoints represented in the librarian's response.
Table 2 Viewpoint example
After categorization, librarians performed an additional analysis within the subset of treatment-related questions (Treatment, Treatment adverse effects, Treatment efficacy) for their units to examine the articles provided in response to each question to assess the number of viewpoints represented. We selected the treatment-related subset based on the assumption that these types of questions would be most likely to require the representation of multiple viewpoints.
Statistical analysis
Frequency distributions were used initially to summarize redundancy, classifications, and viewpoints. Subsequently, these distributions were crosstabulated by clinical unit for analysis of differences in these distributions among the units. The chi-square test statistic was used to assess the statistical significance of these findings (minimum alpha = 0.05).
RESULTS
Between April 1, 1997, and November 30, 1999, CICS librarians answered a total of 547 questions from seven clinical units. Attending physicians submitted 285 questions (52%), residents 158 questions (29%), clinical fellows 64 questions (12%), nurses 17 questions (3%), medical students 11 questions (2%), pharmacists 8 questions (1%), and patients 4 questions (1%).
Redundancy analysis
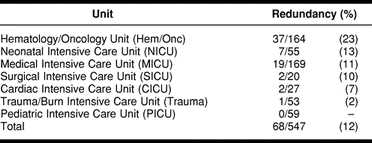
Table 3 illustrates the redundancy rate across the seven units; this rate of repeat questions ranged from 0 (PICU) to 23% (Hem/Onc). Crosstabulation analysis of redundancy distributions revealed a statistically significant difference in redundancy rates among the units (χ2(6) = 30.4, P < 0.001). Hem/Onc had a higher rate of redundancy (P < 0.001) than would be expected from the overall rate, while Trauma and PICU had lower than expected rates (both P < 0.05). Redundant queries were removed, leaving 476 unique queries for subsequent category and viewpoint analyses.
Table 3 Redundancy rates by unit
Category analysis
The results of the category classification are shown in Table 4. The average rate of disagreement in the categorization analysis between the two reviewers for each unit was approximately 6%; all differences were resolved by discussion.
Table 4 Category analysis of questions answered by the Clinical Informatics Consult Service
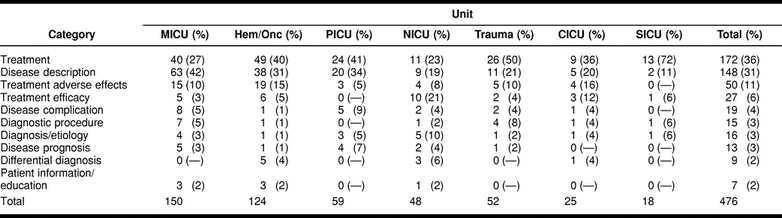
Among all CICS Knowledge Base questions, 320 queries (67%) fell into the top two categories: treatment (36%) and disease description (31%). Treatment-related questions (treatment, treatment adverse effects, treatment efficacy) accounted for 249 questions (52%). The CICS Knowledge Base contained 180 requests (38%) for disease-related information (disease description, disease complication, disease prognosis). Questions regarding diagnosis (diagnosis/etiology, diagnostic procedure, differential diagnosis) accounted for 40 questions (8%). The database contained only 7 requests (7%) for patient information.
Crosstabulation analysis of the category distributions within the units revealed statistically significant interaction between type of question category and unit (χ2(54) = 114.6, P < 0.001). With the exception of SICU (P = 0.64), treatment or disease description categories were used more often than other categories in each unit (CICU: P < 0.01, Hem/Onc: P < 0.001, MICU: P < 0.001, NICU: P < 0.01, PICU: P < 0.001, Trauma: P < 0.01). MICU had more queries about disease description than treatment (P < 0.01), while SICU and Trauma had more queries about treatment than disease description (both P < 0.05). Statistically significant differences were not found between these two types of queries within the other units.
Viewpoint analysis
Two hundred forty-nine treatment-related questions were further analyzed for the number of viewpoints represented in the provided articles. Of the 249 treatment-related questions, twenty-nine questions were answered using general overview material and were excluded from further analysis. CICS librarians were unable to find an answer upon extensive search of the literature for two questions; these questions were also excluded from the viewpoint analysis. Thus, we conducted the analysis of viewpoints in 218 treatment-related questions answered with one or more articles that met the inclusion criteria. Table 5 illustrates the results of the viewpoint analysis.
Table 5 Number of viewpoints provided for treatment-related questions

In this phase of the analysis, we found that 138 questions (59%) required the representation of more than one viewpoint. Twelve questions (6%) were answered with four or more viewpoints. A comparison of differences among the viewpoint distributions within the units was not statistically significant (χ2(18) = 28.3, P = 0.06).
DISCUSSION
This detailed examination of the clinical questions illustrates the role of the information specialist as an integral member of the patient care team. The significant differences among clinical units revealed in the redundancy and category analyses substantiates our perception that each clinical team has unique information needs. CICS librarians provide in-depth representation and synthesis of the medical literature with regard to each question, tailored to the unit and the clinical case at hand.
While clinicians have an obvious imperative to maintain awareness of current research to sustain high-quality patient care, the realities of day-to-day practice may often preclude spending an adequate amount of time answering every clinical question. Internal CICS benchmarking statistics indicate that experienced librarians spend an average of approximately two hours with each question; moreover, they may spend five or more hours working with complex questions that require extensive searching and filtering of the literature. Davidoff and Florance assert, “Physicians don't, and never will, have [one hour or more] to look for the answers to most of their clinical questions themselves” [34]. It is simply not feasible for physicians to devote such a significant amount of time to clinical queries, particularly when we consider that physicians often encounter multiple questions during daily clinical practice [35–38]. Indeed, studies indicate that many questions generated during patient care may never be pursued or answered [39, 40]. Not only do these unanswered questions represent missed opportunities for education and improvement of clinical practice [41], but also “much of the effort, creativity, and money that go into biomedical research is simply wasted” when research fails to inform patient care [42].
Answering questions for which there is no clear consensus in the literature can be particularly time consuming; however, neglecting to locate or examine all possible treatment options, for example, may significantly handicap a clinician's delivery of care. As demonstrated by the viewpoint analysis, if librarians stop searching the literature after finding the first article, additional viewpoints would have been missed in more than half of the treatment-related questions. This situation represents a significant opportunity for librarians, who are generally comfortable with the importance of providing a comprehensive representation of the literature. With high recall as a chief goal and expertise in both searching knowledge and the clinical context, librarians are uniquely positioned to assist clinicians in bridging the gap between the wealth of information available and the incorporation of new knowledge into clinical practice.
The lack of significant differences in the number of represented viewpoints across units supports our belief in the importance of the EBL focus on representation of all views in the literature by CICS librarians regardless of unit.
The category classification illustrates the types of questions for which CICS librarians are consulted by clinical teams. We found that VUMC clinicians use the service most frequently for treatment-related requests—more than half of the questions fall in these categories. Requests for disease-related information account for the bulk of the remaining questions. This prevalence of clinician requests for disease descriptions or treatment information during daily practice is echoed in other discussions of physicians' information needs [43–47].
The initial impetus for construction of the CICS Knowledge Base was to capture the time and expertise that librarians contribute to VUMC clinical units, with the expectation that this resource would become increasingly reusable over time [48]. The redundancy data in the current study emphasizes the value of this reusable resource for both librarians and clinicians. The three highest redundancy rates in the current study occur in the clinical units with the greatest duration of CICS service. Ely et al. note the utility of this type of resource in capturing knowledge and avoiding duplication of effort [49]. As CICS grows, we expect that the trend toward repeated questions will continue and that this tool will become an increasingly important educational resource for our teams. Currently, one unit has taken advantage of this resource by hosting, on its departmental Web page, a dynamic link to that team's past questions and answers in the CICS Knowledge Base. Clinicians rotating onto the unit use this resource as a means of becoming familiar with the librarian's past presentations and acquainting themselves with the team's previous discussions of the medical literature. Librarians on rounds are currently promoting this type of link to all CICS clinical units as a case-based educational opportunity for the teams.
While available time remains an important limitation on clinicians' forays into the medical literature, physicians equipped with a basic level of training in locating and evaluating evidence are able to conduct online database searches with recall comparable to that of librarians [50, 51]. With the goal of utilizing CICS as a mechanism for training clinical team members, we have employed a new CICS model since December 1999. Our initial category analysis indicates that a portion of questions received on rounds are requests for general overview information. For these relatively quick, straightforward queries, CICS librarians now provide resource selection and search strategy assistance tailored to the clinical case rather than a fully filtered information packet. With the understanding that the residents and other clinicians may eventually move to health care environments in which differing levels of library service will be available, we hope to help our clinicians acquire a sound foundation of skills to meet their own basic information needs.
CICS librarians continue to provide searching and synthesis of the literature in response to the more complex queries that may take up to several hours to complete. These questions range from those that require complex search strategies and use of multiple resources to those that require representation of multiple viewpoints to thoroughly represent the current thought on a topic.
Resources that provide varying levels of synthesis of the medical literature with regard to assorted topics, such as the Cochrane Library or UpToDate, have been suggested as a means of promoting the incorporation of research evidence into clinical practice [52, 53]. Though such resources are expanding and becoming more widely available, issues of coverage and maintaining currency remain chief concerns for all evidence-based tools. Incorporated into the framework of the CICS Knowledge Base is a mechanism for updating the records. The librarian who completes the initial CICS packet becomes the owner of the question; daily automated reports identify records for updating every six months. Librarians review the CICS Knowledge Base records for which they are responsible to assess whether new articles should be added to each record. An automated link from the record to the PubMed search strategy created by the librarian provides a quick method for such review and supplies clinicians with an expert strategy for locating additional information on the topic.
As the number of questions in the CICS Knowledge Base continues to grow, we anticipate that the categories will provide convenient access points for clinicians browsing the resource. As new information specialists are trained in CICS, we also expect that this resource will become an integral part of building a subject knowledgebase for work with the various units.
The growth rate of the medical literature, the volume of unpursued clinical questions, and the increasing time constraints faced by clinicians provide a disconcerting picture of knowledge-related issues in current clinical practice. The information specialist is uniquely positioned to assist clinicians in bridging this gap between the medical literature and patient care. As illustrated by this analysis of questions addressed by CICS librarians, trained information specialists working in the clinical context can provide valuable assistance in the practice of evidence-based medicine and function as the “critical link between the huge body of information hidden away in the medical literature and the information needed at the point of care” [54].
Acknowledgments
The authors wish to thank Richard Bankowitz, M.D., for his review of the categories. The authors also gratefully acknowledge the assistance of Marcia Epelbaum, Elizabeth McKinney de Garcia, and Sandi Martin.
REFERENCES
- Patrick SC. Critical appraisal of the medical literature: selected readings. Med Ref Serv Q. 1994 Fall; 13(3):37–7. [Google Scholar]
- Williamson JW, German PS, Weiss R, Skinner EA, and Bowes F. Health science information management and continuing education of physicians. A survey of U.S. primary care practitioners and their opinion leaders. Ann Intern Med. 1989 Jan 15; 110(2):151–60. [DOI] [PubMed] [Google Scholar]
- Hunt RE, Newman RG. Medical knowledge overload: a disturbing trend for physicians. Health Care Manage Rev. 1997 Winter; 22(1):70–5. [PubMed] [Google Scholar]
- MEDLINE fact sheet. . [Web Document]. Bethesda, MD: National Library of Medicine. [4 May 2000; cited 27 Jun 2000]. <http://www.nlm.nih.gov/pubs/factsheets/medline.html>. [Google Scholar]
- Zipser J. MEDLINE to PubMed and beyond. [Web Document]. Presented at the Health Sciences Library Association of New Jersey and New York-New Jersey Chapter of MLA Joint Meeting, Princeton, NJ, December 8, 1999. [10 Aug 1999; cited 27 Jun 2000]. <http://www.nlm.nih.gov/bsd/historypresentation.html>. [Google Scholar]
- Wyatt J. Use and sources of medical knowledge. Lancet. 1991 Nov 30; 338(8779):1368–73. [DOI] [PubMed] [Google Scholar]
- Sackett DL, Rosenberg WM, Gray JA, Haynes RB, and Richardson WS. Evidence based medicine: what it is and what it isn't. BMJ. 1996 Jan 13; 312(7023):71–2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Scherrer CS, Dorsch JL. The evolving role of the librarian in evidence-based medicine. Bull Med Libr Assoc. 1999 Jul; 87(3):322–8. [PMC free article] [PubMed] [Google Scholar]
- McKibbon KA. Evidence-based practice. Bull Med Libr Assoc. 1998 Jul; 86(3):396–401. [PMC free article] [PubMed] [Google Scholar]
- Giuse NB. Advancing the practice of clinical medical librarianship [editorial]. Bull Med Libr Assoc. 1997 Oct; 85(4):437–8. [PMC free article] [PubMed] [Google Scholar]
- Giuse NB, Kafantaris SR, Miller MD, Wilder KS, Martin SL, Sathe NA, and Campbell JD. Clinical medical librarianship: the Vanderbilt experience. Bull Med Libr Assoc. 1998 Jul; 86(3):412–6. [PMC free article] [PubMed] [Google Scholar]
- Wilder KS, Jerome R, Giuse NB, Williams MD, Martin S, and Epelbaum M. Using the products of clinical librarianship to design a medical knowledge base. Paper presented at: Ninety-ninth Medical Library Association Annual Meeting; Chicago, IL, May 18, 1999 [Google Scholar]
- Cimpl K. Clinical medical librarianship: a review of the literature. Bull Med Libr Assoc. 1985 Jan; 73(1):21–8. [PMC free article] [PubMed] [Google Scholar]
- Halsted DD, Ward DH, and Neeley DM. The evolving role of clinical medical librarians. Bull Med Libr Assoc. 1989 Jul; 77(3):299–301. [PMC free article] [PubMed] [Google Scholar]
- Demas JM, Ludwig LT. Clinical medical librarian: the last unicorn? Bull Med Libr Assoc. 1991 Jan; 79(1):17–27. [PMC free article] [PubMed] [Google Scholar]
- Veenstra RJ. Clinical medical librarian impact on patient care: a one-year analysis. Bull Med Libr Assoc. 1992 Jan; 80(1):19–22. [PMC free article] [PubMed] [Google Scholar]
- Kuller AB, Wessel CB, Ginn DS, and Martin TP. Quality filtering of the clinical literature by librarians and physicians. Bull Med Libr Assoc. 1993 Jan; 81(1):38–43. [PMC free article] [PubMed] [Google Scholar]
- Royal M, Grizzle WE, Algermissen V, and Mowry RW. The success of a clinical librarian program in an academic autopsy pathology service. Am J Clin Pathol. 1993 May; 99(5):576–81. [DOI] [PubMed] [Google Scholar]
- Marshall JG. Issues in clinical information delivery. Libr Trends. 1993 Summer; 42(1):83–107. [Google Scholar]
- Matheson NW. The idea of the library in the twenty-first century. Bull Med Libr Assoc. 1995 Jan; 83(1):1–7. [PMC free article] [PubMed] [Google Scholar]
- Giuse NB. Advancing the practice of clinical medical librarianship [editorial]. Bull Med Libr Assoc. 1997 Oct; 85(4):437–8. [PMC free article] [PubMed] [Google Scholar]
- Giuse NB, Kafantaris SR, Miller MD, Wilder KS, Martin SL, Sathe NA, and Campbell JD. Clinical medical librarianship: the Vanderbilt experience. Bull Med Libr Assoc. 1998 Jul; 86(3):412–6. [PMC free article] [PubMed] [Google Scholar]
- Giuse NB. Advancing the practice of clinical medical librarianship [editorial]. Bull Med Libr Assoc. 1997 Oct; 85(4):437–8. [PMC free article] [PubMed] [Google Scholar]
- Gorman PN, Helfand M. Information seeking in primary care: how physicians choose which clinical questions to pursue and which to leave unanswered. Med Decis Making. 1995 Apr; 15(2):113–9. [DOI] [PubMed] [Google Scholar]
- Verhoeven AAH, Boerma EJ, and Meyboom-de Jong B. Use of information sources by family physicians: a literature survey. Bull Med Libr Assoc. 1995 Jan; 83(1):85–90. [PMC free article] [PubMed] [Google Scholar]
- Haug JD. Physicians' preferences for information sources: a meta-analytic study. Bull Med Libr Assoc. 1997 Jul; 85(3):223–32. [PMC free article] [PubMed] [Google Scholar]
- Smith R. What clinical information do doctors need? BMJ. 1996 Oct 26; 313(7064):1062–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giuse NB, Kafantaris SR, Miller MD, Wilder KS, Martin SL, Sathe NA, and Campbell JD. Clinical medical librarianship: the Vanderbilt experience. Bull Med Libr Assoc. 1998 Jul; 86(3):412–6. [PMC free article] [PubMed] [Google Scholar]
- Haynes B, Haines A. Barriers and bridges to evidence based clinical practice. BMJ. 1998 Jul 25; 317(7153):273–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giuse NB, Kafantaris SR, Miller MD, Wilder KS, Martin SL, Sathe NA, and Campbell JD. Clinical medical librarianship: the Vanderbilt experience. Bull Med Libr Assoc. 1998 Jul; 86(3):412–6. [PMC free article] [PubMed] [Google Scholar]
- Matheson NW. The idea of the library in the twenty-first century. Bull Med Libr Assoc. 1995 Jan; 83(1):1–7. [PMC free article] [PubMed] [Google Scholar]
- Davidoff F, Florance V. The informationist: a new health profession? Ann Intern Med. 2000 Jun 20; 132(12):996–8. [DOI] [PubMed] [Google Scholar]
- Giuse NB, Huber JT, Giuse DA, Brown CW, Bankowitz RA, and Hunt S. Information needs of health care professionals in an AIDS outpatient clinic as determined by chart review. J Am Med Inform Assoc. 1994 Sep; 1(5):395–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davidoff F, Florance V. The informationist: a new health profession? Ann Intern Med. 2000 Jun 20; 132(12):996–8. [DOI] [PubMed] [Google Scholar]
- Giuse NB, Huber JT, Giuse DA, Brown CW, Bankowitz RA, and Hunt S. Information needs of health care professionals in an AIDS outpatient clinic as determined by chart review. J Am Med Inform Assoc. 1994 Sep; 1(5):395–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Covell DG, Uman GC, and Manning PR. Information needs in office practice: are they being met? Ann Intern Med. 1985 Oct; 103(4):596–9. [DOI] [PubMed] [Google Scholar]
- Osheroff JA, Forsythe DE, Buchanan BG, Bankowitz RA, Blumenfeld BH, and Miller RA. Physicians' information needs: analysis of questions posed during clinical teaching. Ann Intern Med. 1991 Apr 1; 114(7):576–81. [DOI] [PubMed] [Google Scholar]
- Forsythe DE, Buchanan BG, Osheroff JA, and Miller RA. Expanding the concept of medical information: an observational study of physicians' information needs. Comput Biomed Res. 1992 Apr; 25(2):181–200. [DOI] [PubMed] [Google Scholar]
- Gorman PN, Helfand M. Information seeking in primary care: how physicians choose which clinical questions to pursue and which to leave unanswered. Med Decis Making. 1995 Apr; 15(2):113–9. [DOI] [PubMed] [Google Scholar]
- Ely JW, Osheroff JA, Ebell MH, Bergus GR, Levy BT, Chambliss ML, and Evans ER. Analysis of questions asked by family doctors regarding patient care. BMJ. 1999 Aug 7; 319(7206):358–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gorman PN, Helfand M. Information seeking in primary care: how physicians choose which clinical questions to pursue and which to leave unanswered. Med Decis Making. 1995 Apr; 15(2):113–9. [DOI] [PubMed] [Google Scholar]
- Davidoff F, Florance V. The informationist: a new health profession? Ann Intern Med. 2000 Jun 20; 132(12):996–8. [DOI] [PubMed] [Google Scholar]
- Smith R. What clinical information do doctors need? BMJ. 1996 Oct 26; 313(7064):1062–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Giuse NB, Huber JT, Giuse DA, Brown CW, Bankowitz RA, and Hunt S. Information needs of health care professionals in an AIDS outpatient clinic as determined by chart review. J Am Med Inform Assoc. 1994 Sep; 1(5):395–403. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Osheroff JA, Forsythe DE, Buchanan BG, Bankowitz RA, Blumenfeld BH, and Miller RA. Physicians' information needs: analysis of questions posed during clinical teaching. Ann Intern Med. 1991 Apr 1; 114(7):576–81. [DOI] [PubMed] [Google Scholar]
- Ely JW, Osheroff JA, Ebell MH, Bergus GR, Levy BT, Chambliss ML, and Evans ER. Analysis of questions asked by family doctors regarding patient care. BMJ. 1999 Aug 7; 319(7206):358–61. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lindberg DA, Siegel ER, Rapp BA, Wallingford KT, and Wilson SR. Use of MEDLINE by physicians for clinical problem solving. JAMA. 1993 Jun 23; 269(24):3124–9. [PubMed] [Google Scholar]
- Giuse NB, Kafantaris SR, Miller MD, Wilder KS, Martin SL, Sathe NA, and Campbell JD. Clinical medical librarianship: the Vanderbilt experience. Bull Med Libr Assoc. 1998 Jul; 86(3):412–6. [PMC free article] [PubMed] [Google Scholar]
- Ely JW, Osheroff JA, Ferguson KJ, Chambliss ML, Vinson DC, and Moore JL. Lifelong self-directed learning using a computer database of clinical questions. J Fam Pract. 1997 Oct; 45(5):382–8. [PubMed] [Google Scholar]
- Haynes RB, McKibbon KA, Walker CJ, Ryan N, Fitzgerald D, and Ramsden MF. Online access to MEDLINE in clinical settings. a study of use and usefulness. Ann Intern Med. 1990 Jan 1; 112(1):78–84. [DOI] [PubMed] [Google Scholar]
- Hersh W, Hickam D. Use of a multi-application computer workstation in a clinical setting. Bull Med Libr Assoc. 1994 Oct; 82(4):382–9. [PMC free article] [PubMed] [Google Scholar]
- Haynes B, Haines A. Barriers and bridges to evidence based clinical practice. BMJ. 1998 Jul 25; 317(7153):273–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davidoff F, Florance V. The informationist: a new health profession? Ann Intern Med. 2000 Jun 20; 132(12):996–8. [DOI] [PubMed] [Google Scholar]
- Davidoff F, Florance V. The informationist: a new health profession? Ann Intern Med. 2000 Jun 20; 132(12):996–8. [DOI] [PubMed] [Google Scholar]