

Abstract
Neonatal hypoxic-ischemic encephalopathy (HIE) is a clinically defined neurological condition following lack of oxygen and often associated with cardiac dysfunction in term infants. Therapeutic hypothermia after birth is neuroprotective in infants with HIE. However, it is not known whether hypothermia (HT) is also cardioprotective. Four newborn pigs were used in the pilot study and a further 18 newborn pigs (randomly assigned to 72h-normothermia (NT) or 24h-HT followed by 48h-NT) were subjected to global HIE insults. Serum cTnI was measured prior to and post the HIE insult. Blood pressure, inotropic support, blood gases and heart rate (HR) were recorded throughout. Cardiac pathology was assessed from histological sections. Cooling reduced serum cTnI levels significantly in HT pigs by 6h (NT, 1.36±0.67; HT 0.34±0.23 ng/ml, p=0.0009). After rewarming, from 24 to 30h post insult, HR and cTnI increased in the HT group; from HR[24h]=117±22 to HR[30h]=218±32 beats/minute (p=0.0002) and from cTnI[24h]=0.23±0.12 to cTnI[30h]=0.65±0.53ng/ml, (p=0.05). There were fewer ischemic lesions on cardiac examination (37%) in the HT group compared to the NT group (70%). Hypothermia (24h) pigs did not have the post-insult cTnI increase seen in NT treated pigs. There was a trend that HT improved cardiac pathology in this 3-day survival model.
Introduction
Severe lack of oxygen or perfusion around the time of birth (perinatal asphyxia) leads to hypoxic-ischemic encephalopathy (HIE) and is associated with significant mortality and long-term morbidity. Hypoxic-ischemic encephalopathy is characterised by clinical and laboratory evidences of brain injury associated with hypoxia and acidosis. Neonatal HIE affects up to 6 per 1000 live births (1). In an autopsy study, cardiac injury is the most prominent organ injury (62%) in addition to brain injury (2). Therapeutic hypothermia (HT) after birth (cooling of core temperature to 33-34°C for 72 hours) improves neurological outcome at 18 months of age in this group of patients (3-5). There is no direct evidence to show that therapeutic HT is also cardio-protective in newborns with HIE. In asphyxiated cooled newborns, hypothermia has been shown to induce mild sinus bradycardia and a slight increase in mean arterial blood pressure (MABP) (6). Whether such cardiovascular changes confer protection against hypoxia is not presently known.
Cardiac troponins (cTnT and cTnI) are proteins released from injured cardiomyocytes. They are established biological markers with high sensitivity to diagnose myocardial cell injury in adults (7, 8) and neonates (9, 10). Furthermore, the level of cTnI in cord blood has been suggested to predict early mortality after perinatal asphyxia (11). The aim of this study is to determine whether immediate cooling after the acute insult is cardioprotective in an established hypoxic-ischemic newborn pig model (12).
Methods
All animal work was carried out and approved under Home Office license in accordance with UK guidelines. This study was approved by the Animal Ethical Review Panel at the University of Bristol. Twenty-two crossbred Landrace large white newborn pigs of either sex, median (interquartile range, IQR) age of 18h (9-20) and median weight of 1.64kg (1.4-1.8) were used in this study. Four pigs were used in the pilot study and 18 pigs were used in the experimental study (normothermia (NT) =10, HT=8).
Global hypoxic-ischaemic insult
All animals were subjected to our established global hypoxic-ischaemic insult (HI) (12, 13). Briefly, unrestrained animals were anaesthetised with 4.0% halothane and nitrous oxide (N2O) in a closed Perspex box followed by intubation and mechanical ventilation with halothane 0.7%, N2O 65%, and oxygen ~ 35%. Ventilator settings were adjusted to maintain end-tidal carbon dioxide around 5.3 ±0.3 kPa during the study, but PCO2 were kept unadjusted during the 45 minutes insult. Hypoxic-ischaemic injury was introduced by rapidly reducing the fraction of inspired oxygen concentration (FiO2) to 4-6% in a gas mixture (nitrogen and oxygen) for 45 minutes. Consequently, the continuously recorded electroencephalogram(EEG) became depressed (<7μV) for at least 20 minutes (12) accompanied by hypotension (mean blood pressure <40mmHg). Animals were resuscitated with appropriate FiO2 (starting from air), avoiding hyperoxia, to maintain transcutaneous oxygen saturation (TcSaO2) between 95-98% (Masimo SET, Masimo Corporation, California, USA). Previously (12), we resuscitated pigs with 100%O2 and corrected acidosis with bicarbonate. Since 2003 (13), we have resuscitated pigs with air and followed clinical guidelines increasing in steps of +5% O2 every 90 seconds if the saturation did not improve. Typically, no more than 30% oxygen was used to resuscitate a pig after the insult.
Before and during the insult newborn pigs were kept NT at 39°C which is a normal body temperature for newborn pigs (14, 15). After the insult, pigs were kept either NT for 72h or HT at 34.5°C for the first 24h followed by 48h NT until sacrificed at 72h post insult.
Pilot experiments
Newborn pigs, unlike humans, have low haemoglobin at birth (~8g/dL) and frequent blood sampling will make them anaemic. Therefore, to decide the minimum frequency and the best sampling time-points for cTnI after the insult, a small pilot experiment (4 pigs with mild HI insult) with frequent blood sampling (baseline, 1h,3h,6h,12h,24h,48h and 72h post insult) at NT were carried out. In Fig 1, cTnI was measured before the insult and at the set time points after the insult and cTnI visually peaks at 3-6h. We chose to measure the first cTnI at 6h in our main study to minimize sampling frequency to 6 including the peak cTnI value.
Figure 1.
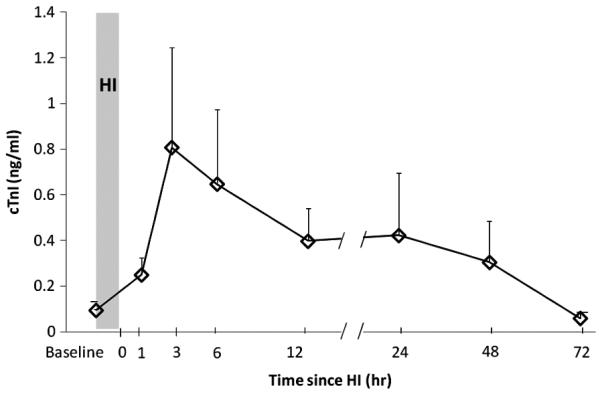
Frequent serum cardiac troponin I levels (mean±SEM) in 4 pilot pigs that underwent 45 min of global hypoxia-ischemia and then kept at normothermia for 72 hours to characterize the time course of cTnI changes.
Anaesthesia
Umbilical arterial and venous catheters were inserted to allow for continuous MABP monitoring (Philips, USA), repeated blood sampling and infusion of fluids and drugs. After the insult, inhalation anaesthesia was changed to intravenous anaesthesia. Bolus doses of Propofol (4mg/kg) and Fentanyl (30μg/kg) were followed by maintenance infusions of 4-12 mg/kg/h Propofol and 10μg/kg/h Fentanyl. Twenty-four hours after the insult (equivalent to the end of cooling), maintenance anaesthesia was stopped, rewarming started in the HT groups and pigs from both groups were allowed to wake up and be extubated when breathing independently. We have previously shown that pigs were stressed with high heart rate (HR) and cortisol levels if kept awake and cold during HT treatment (16).
The cumulative amount of Propofol and Fentanyl given in the HT and NT groups did not differ. Fentanil was given at 10mcg/kg/h in both groups and propofol at 4.9mg/kg/h in the HT and 5.6mg/kg/h in the NT group.
Therapeutic hypothermia and normothermia
Pigs in the NT group were maintained throughout the study period at the target rectal temperature 39.0±0.2°C for 72h. Pigs in the HT group were cooled immediately after the insult for 24h using a cooling cap (The Cool Care System, Natus, Seattle, USA) combined with mild body HT to rectal temperature 34.5°C for 24h. An overhead infant heater was used to ensure a stable core temperature (4, 17). At the end of the HT treatment, pigs were rewarmed over 6h to a rectal temperature of 39°C. All pigs received standard intensive care. Blood pressure, HR and continuous EEG were monitored. If a single seizure (both clinical and electrical) lasted more than 10 minutes, a loading dose of Phenobarbitone at 20mg/kg was given over 20 minutes. A second dose of phenbarbitone was given if there was no effect within 60 minutes from the first dose. A third anticonvulsant, clonazepam, was given at 100μg/kg if needed. Most pigs had electrical seizures (75% in the HT group and 90% in the NT group). The total duration (median, IQR) of EEG seizures is 42 (9-262) minutes in the HT group and 348 (250-423) minutes in the NT group during the 72 hours experimental period. No HT pigs needed any anticonvulsant as the seizure epochs were <10 minutes. Eight/ 10 NT pigs were treated with anticonvulsants. Five of them received one dose of phenobarbitone, 2 required the second dose of phenbarbitone and one pig needed additional clonazepam. Four out of 10 NT pigs received inotropic support and also required anticonvulants.
Mean arterial blood pressure and heart rate monitoring
Continuous MABP was measured from the umbilical artery catheter. During the insult, no lower limit for MABP was set (unless it was associated with increasing bradycardia and prone to cardiac arrest), otherwise a MABP <40mmHg was treated with a 10ml/kg bolus of 0.9% normal saline followed, if the MABP remained low, by a 10ml/kg bolus of 5% human albumin. If hypotension continued, inotropic support was commenced with an infusion of dopamine (range 5-20 μg/kg/min) and then (if necessary) an infusion of noradrenaline (range 0.05-0.1 μg/kg/min). Inotropic support was weaned if the pig’s MABP remained above 45mmHg for 60 minutes. Heart rate was calculated from electrocardiographic (ECG) signals.
cTnI analysis
Blood samples for cTnI measurements were collected at baseline (30 minutes before HI) and at pre-designed time points after HI (6, 12, 24, 30 and 48h post-insult). Serum was stored at −80°C until analysed. Concentrations of cTnI were measured using the ACCESS Immunoassay system (Beckman Instruments Inc. Buckinghamshire UK) which has a low detection limit of 0.01ng/ml.
Histology assessment
Animals were euthanized 72h after HI and the brains were perfusion-fixed using 4% phosphate-buffered formaldehyde (PBF). The hearts were immersion fixed and stored in 4% PBF. The right brain hemisphere of each pig was cut into thirteen 3 mm thick coronal blocks and the heart was cut into five 3 mm thick transverse blocks. Specimens were then dehydrated and paraffin embedded. Sections (6 μm) were cut and stained with haematoxylin and eosin.
The clinical pathologists who assessed the sections under light microscopy were blinded to the treatment groups. A modified scoring system (18, 19) was used for the heart based on the type and the total number of lesions counted in 5 cross sections from each heart. The brain injury score system in our model (9-step with intervals of 0.5 from 0.0 to 4.0 from 6 brain regions) has been presented and validated previously (12).
Statistical Analysis
Descriptive data is presented with mean ± Standard Deviation (SD) or median ± IQR. A student t test was performed to compare means of two cTnI levels. The ‘N-1’ chi squared test was used to compare cardiac pathology data (20). Linear regression was carried out to define the relations between serum cTnI levels and heart or brain pathology scores using SPSS v16.
Results
The severity of the HI insult was similar in both groups defined by the duration of depressed (low amplitude <7μV) EEG, the pH and Base Excess (BE) at the end of HI and percentage of time the blood pressure fell below 40mmHg during HI (13). The average MABP during the insult was 38 ± 5.1 mmHg in the NT and 33± 4.5 mmHg in the HT pigs. . Values of arterial pH and BE at the end of HI were similar in the NT and HT groups; 7.01 ± 0.036 in NT compared to 7.11 ±0.062 in HT, and −21.4±2.3in the NT vs −24.7± 3.1mmol/L in the HT pigs. Demographic data are shown in Table 1.
Table 1.
demographic values in the two experimental groups during the insult.
| Group | Treatment | P value | |
|---|---|---|---|
| Normothermia (n=10) | Hypothermia (n=8) | ||
|
Age (hours) median,
IQR) |
18 (6-30) | 13.5 (2-24) | 0.31 |
| Weight (kg, median IQR) | 1.63 (1.09-2.17) | 1.60 (1.29-1.91) | >0.5 |
|
Duration of aEEG <7μv during HI (min) |
29.7±9 | 25.2±8.4 | >0.5 |
|
pH at the end of HI
(mean±SD) |
7.01±0.036 | 7.11±0.062 | 0.18 |
|
Base Excess at the end
of HI (mmol/L,mean±SD) |
−21.4±2.3 | −24.7±3.1 | >0.5 |
|
MABP during the insult
(mmHg) |
38±5.1 | 33±4.5 | >0.5 |
aEEG: amplitude-integrated EEG
cTnI release in hypoxic pigs
Baseline cTnl levels were similar between the NT and HT groups; 0.14 (0.07-0.33) ng/ml in NT pigs vs. 0.13 (0.06-0.25) ng/ml in HT pigs (p=0.80). It is also consistent with our pilot experiment which indicated that the cut off value of cTnI for a newborn pig is below 0.2ng/ml. At 6h post insult, a significant rise in cTnI levels from baseline was seen in both NT and HT groups (fig 2). Importantly, the peak rise was 3 times greater in the NT group than the HT group (cTnI[NT]=1.36 ± 0.67ng/ml and cTnI[HT]=0.34 ± 0.23ng/ml, p=0.0009). By the end of 6h rewarming and discontinuation of anaesthesia (30h after the insult), there was a transient increase (p=0.05; HT group) in cTnI in both groups before falling back to baseline levels at 48h after insult. There was a concomitant 100% rise in heart rate in the HT group between 24 and 30h during rewarming.
Figure 2.
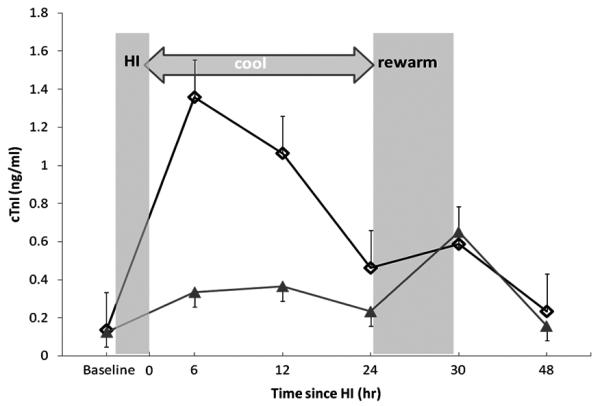
Mean± SEM cardiac troponin I levels in animals treated with normothermia ( ; n=10) and hypothermia (▲; n=8) at baseline, 6h, 12h, 24h, 30h and 48h after the 45-min hypoxic-ischemia insult.
; n=10) and hypothermia (▲; n=8) at baseline, 6h, 12h, 24h, 30h and 48h after the 45-min hypoxic-ischemia insult.
Blood pressure and heart rate in NT and HT treated newborn pigs
There was no statistical difference in MABP between NT and HT treated animals (fig3). There was no difference in the use of inotropic drugs (dopamine and noradrenaline) between the two groups, 50% HT and 40% NT pigs received inotropic support. The average of duration of inotropic support was 1092 ±419 minutes in the HT group and 1690 ±1092 minutes in the NT group (p=0.4). The accumulated dopamine dosage was 14.4±6.3 mcg/kg/min in the HT group and 15.6±9.6 mcg/kg/min in the NT group (p=0.4). Only one HT pig had noradrenaline for five hours.
Figure 3.
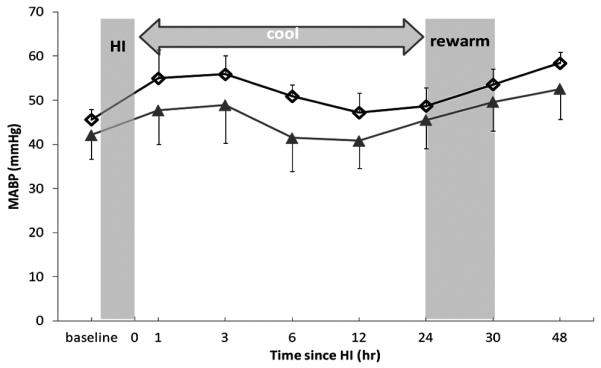
Mean± SEM blood pressure in normothermia (; n=10) and hypothermia (▲; n=8) treated animals at baseline, 3h, 6h, 12h, 24h, 30h and 48h after the 45-min hypoxic-ischemia insult.
There was a significant difference in the heart rate between the NT and HT groups during the first 24h (hypothermia period (p<0.001) (fig4a). There was a dramatic increase in heart rate during rewarming in the HT group (HR[24h]= 117±22 beats/min; HR[30h]= 218±32 beats/min; p= 0.0002) but no increase in the NT group at 24-30h when anaesthesia was discontinued in both groups (fig4b). We did not find any major adverse events such as hypotention, bradycardia, arrhythmia and pulmonary hypertension in this study. There was no increased oxygen requirement in the cooled group. This is consistent with a recent meta-analysis of 3 large neonatal cooling trials (21).
Figure 4.

(A) Mean± SEM heart rate in normothermia (; n=10) and hypothermia (▲; n=8) treated animals at baseline, 3h, 6h, 12h, 24h, 30h and 48h after the 45-min hypoxic-ischemia insult. (B)shows the correlation between heart rate and cardiac troponin I at the end of cooling (24h, ▲) and end of rewarming (30h, Δ) in the cooled group (HT n=8). Different styles of lines linking two time points (24h and 30h) are used to separate individual changes in animals.
Effect of hypothermia on myocardial structural changes during HIE
Histological injury of the heart was observed in 70% of the NT group compared to 37% in the HT group. There were no large infarcts, only multiple smaller lesions. These lesions consisted of a varying amount of necrotic muscle fibres surrounded by a cellular reactive reaction. Most (89%) lesions were localized sub-endocardially in the right ventricle regardless of treatments (fig5a).
Figure 5.

(A-B) representative images of an injured newborn pig heart at magnifications at 200X (panel a, bar= 200μm) and magnifications at 400X (panel b, bar= 100μm). The magnified image (B) on the right bottom of the corner represents a small myocardial infarct with eosinophilic myocytes with pyknotic or disintegrated nuclei. (C) The correlation between the level of cardiac troponin I at 6h after HI and the number of pathologcal lesions in the heart in the normothermia (NT) group. Normothermia (; n=10); hypothermia (▲; n=8).
There was a trend for having reduced number of lesions in animals treated with HT compared to NT (p=0.07) (fig5c).The 6h-post HI cTnI level correlated well with the number of lesion in the heart in the NT groups but not in the HT group (r2[NT]=0.35, p=0.07; r2[HT]=0.019, p=0.74)(fig5c).
The 6h-post HI cTnI concentration correlated with brain pathology score at 72h when combining both groups but not with individual treatment groups (r2[NT+HT] =0.39, p=0.005;r2[NT]=0.26, p=0.13; r2[HT]=0.036,p=0.65) (fig6).
Figure 6.
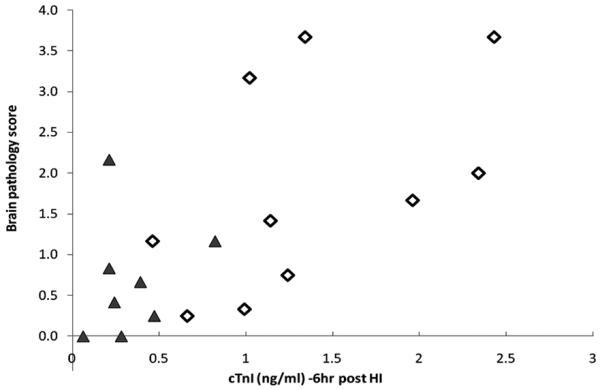
The levels of cardiac troponin I at 6h after the insult are plotted against the average brain pathology score at 72h after the insult. Normothermia (; n=10); hypothermia (▲; n=8).
Discussion
This work presents, for the first time, that therapeutic hypothermia following hypoxia-ischemia in newborn pigs is also cardioprotective in our established newborn pig global HIE model. This global injury model of neonatal brain injury with multi-organ failure was used in neuroprotective cooling research (13, 16, 22-24) and contributed towards successful clinical trials (3, 4). Increasingly, therapeutic hypothermia is becoming standard of care in treating HIE infants worldwide(25). Hypothermia has proven to be neuroprotective, but there is no sufficient evidence demonstrating whether HT confers cardioprotection in intensive care patients. Some concern relates to work on adults where hypothermia treatment causes hypotension (26). However, hypotension during 3 days of HT treatment was not found in 3 large neonatal clinical hypothermia trials with appropriate care (3-5).
The significant heart rate reduction in the cooling group may confer reduced stress and be an indirect measure of reduced energy and metabolic demand in our study. Our study has followed a strict protocol to treat hypotension and to avoid other adverse incidents. We have introduced background sedation which reduce the stress level during HT treatment (13). We have also previously shown that hypothermia and sedations per se do not increase the apoptotic cell death in our model (27). These may all contribute to hypothermic cardioprotection. We did not see the differences in MABP and in use of inotropics in the first 3 days between the two groups. There is however a trend of a lower MABP in the HT group. In this study, there was only one HT pig which had severe and also drug resistant hypotension during the whole experimental period. Despite this long lasting low MABP, this HT pig only had two ischemic lesions in the heart. The rest of the HT pigs all had MABP >40mmHg during the experiment. Clinically, maintained MABP and reduced use of inotropic support are often noted as signs of cardiac recovery. We did see reduced cTnI levels and improved pathology in the heart in the cooled group which indicated the hypothermic cardiac-protection. It is not possible to obtain the data on heart pathology clinically but cTnI can be used as an early marker to describe injury and cardiac recovery in asphyxia infants.
Cardiac troponin I as a cardiac biomarker is well established in adults and has been recognised as not only a diagnostic but prognostic marker (8). However, its potential application in neonatal medicine has not been fully explored. Cord cTnI was suggested as a good early predicator of severity of HIE in term infants (11). The levels of cTnI are barely detectable in healthy adults and increases in cTnI above the 99th percentile reference limit are considered an indication of myocardial injury. This limit has been reported as low as 0.03ng/ml in adults (28). Comparing cTnI in adults with infants, higher baseline levels of cTnI (>0.03ng/ml)are observed in the first 3 months of life (29). According to our pilot study and the specific cTnI assay used, we have set the normal range of cTnI for a new born pig is below 0.2ng/ml.
In animal studies, it has been reported that the level of cTnI starts to increase by 30 min with a peak value at 3h after cardiac arrest in adult pigs (30) and started to rise from 0.5-1h after induced cardiac injury and normalized within 48h after the insult in adult rodents (31). Our data confirms this rapid release of cTnI after acute injury as we observed the first rise in cTnI at 1h after a 45-min global (Fig 1) insult with a peak around 3-6h in the pilot study. The time course of cTnI release in our normothermic animals is similar to that seen in older children after acute myocardial injury (32). We have also shown the level of cTnI normalised in both treated groups 48 hours after the insult. Similar data for cooled/non-cooled newborns are only available at the age of 72 hours (33) where there was also no difference observed between two groups. In this randomised study, we showed earlier time points after an acute injury. There was a nearly 9-fold cTnI increase 6h after HI and no increase in heart rate or cTnI in the NT pigs when intravenous anaesthesia was ended during the rewarming period. The findings from the HT group are different. In these anaesthetised cooled pigs, the cTnI was much lower in the cooled group compared to NT group. This suggests that hypothermia may provide cellular protection to the heart. Due to small numbers we did not reach significance when comparing the pathology results. Neonatal hearts, different from adult hearts, rely on anaerobic metabolism. They have high glycogen stores. Therefore, neonatal heart has increased tolerance to transient hypoxic-ischemic damage (34). Cardiac troponin I is a more sensitive biomarker compared to cardiac pathology. We may see the transient increase in cTnI without permanent damage in the heart. Additionally, neonatal hearts is better at cellular repair than adult hearts. This may explain that we only see smaller lesions in a subset of animals but a huge increase of cTnI level soon after the insult. During fast rewarming (near 0.8°C/hr) in the HT group, the heart rate almost doubled and there was a significant increase in cTnI which may indicate cardiac stress. The NT pigs had longer durations of seizures. Seizure activity may also increase HR and cardiac stress. Slow rewarming rates may be beneficial for the heart.
In the normothermic newborn pigs after a HI insult, we find a strong relationship between myocardial damage and peak cTnI levels. Prospective clinical data is needed to examine whether cTnI is a valid predictor of neurological/cardiac outcome for HIE infants after therapeutic hypothermia.
There are some limitations to our study. The experimental insult was not carried out around the time of birth but within 24h of age. To introduce HI in our newborn pig model, pigs were ventilated and sedated with halothane for 45 minutes. Clinically, the fetus or newborn may have different types and degree of injury due to the time of the onset and the duration of the insult(s). Some infants may have one prolonged systemic HI injury as demonstrated in our model and others may have a few but shorter episodes of insults that may affect the heart differently. Most injuries were seen in the right ventricle which is a typical location in the newborn stressed heart (35). We used 24 hours cooling treatment in this study which is different from 72 hours applied clinically. Different animal species require different effective cooling durations. We have previously shown that 24 hours cooling provides better neuroprotection than 12 hours cooling and significant neuroprotection than normothermia (36) in this model. Therefore, we believe 24 hours cooling is the optimal cooling duration in newborn pigs.
In conclusion, mild immediate hypothermia as a post-insult neuroprotective intervention may also protect the heart, in particular if conducted with appropriate clinical management; a slow rewarming rate and with adequate sedation during cooling therapy.
Acknowledgement
We are grateful to Olympic Medical for the CoolCap system, SLE Ltd. for lending us ventilators and Ohmeda Ltd. for the Giraffe incubator.
Funding Sources: The Welcome Trust (UK) and Laerdal Foundation for Acute Medicine (Norway).
Abbreviations
- cTn
cardiac troponin
- HIE
hypoxic-ischemic encephalopathy
- HI
hypoxic-ischemic insult
- HR
heart rate
- HT
hypothermia
- IQR
interquartile range
- MABP
mean arterial blood pressure
- NT
normothermia
Footnotes
Publisher's Disclaimer: Pediatric Research Articles Ahead of Print contains articles in unedited manuscript form that have been peer-reviewed and accepted for publication. As a service to our readers, we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting and review of the resulting proof before it is published in its final definitive form. Please note that during the production process errors may be discovered, which could affect the content, and all legal disclaimers that apply to the journal pertain.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Shankaran S. Neonatal encephalopathy: treatment with hypothermia. J Neurotrauma. 2009;26:437–443. doi: 10.1089/neu.2008.0678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Barnett CP, Perlman M, Ekert PG. Clinicopathological correlations in postasphyxial organ damage: a donor organ perspective. Pediatrics. 1997;99:797–799. doi: 10.1542/peds.99.6.797. [DOI] [PubMed] [Google Scholar]
- 3.Azzopardi DV, Strohm B, Edwards AD, Dyet L, Halliday HL, Juszczak E, Kapellou O, Levene M, Marlow N, Porter E, Thoresen M, Whitelaw A, Brocklehurst P. Moderate hypothermia to treat perinatal asphyxial encephalopathy. N Engl J Med. 2009;361:1349–1358. doi: 10.1056/NEJMoa0900854. [DOI] [PubMed] [Google Scholar]
- 4.Gluckman PD, Wyatt JS, Azzopardi D, Ballard R, Edwards AD, Ferriero DM, Polin RA, Robertson CM, Thoresen M, Whitelaw A, Gunn AJ. Selective head cooling with mild systemic hypothermia after neonatal encephalopathy: multicentre randomised trial. Lancet. 2005;365:663–670. doi: 10.1016/S0140-6736(05)17946-X. [DOI] [PubMed] [Google Scholar]
- 5.Shankaran S, Laptook AR, Ehrenkranz RA, Tyson JE, McDonald SA, Donovan EF, Fanaroff AA, Poole WK, Wright LL, Higgins RD, Finer NN, Carlo WA, Duara S, Oh W, Cotten CM, Stevenson DK, Stoll BJ, Lemons JA, Guillet R, Jobe AH. Whole-body hypothermia for neonates with hypoxic-ischemic encephalopathy. N Engl J Med. 2005;353:1574–1584. doi: 10.1056/NEJMcps050929. [DOI] [PubMed] [Google Scholar]
- 6.Lista G, Pogliani L, Fontana P, Castoldi F, Compagnoni G. Cardiovascular and respiratory status in mechanically ventilated asphyxiated term infants: comparison between hypothermic and control group. Acta Biomed. 2004;75:107–113. [PubMed] [Google Scholar]
- 7.Falahati A, Sharkey SW, Christensen D, McCoy M, Miller EA, Murakami MA, Apple FS. Implementation of serum cardiac troponin I as marker for detection of acute myocardial infarction. Am Heart J. 1999;137:332–337. doi: 10.1053/hj.1999.v137.92412. [DOI] [PubMed] [Google Scholar]
- 8.Inbar R, Shoenfeld Y. Elevated cardiac troponins: the ultimate marker for myocardial necrosis, but not without a differential diagnosis. Isr Med Assoc J. 2009;11:50–53. [PubMed] [Google Scholar]
- 9.Rajakumar PS, Bhat BV, Sridhar MG, Balachander J, Konar BC, Narayanan P, Chetan G. Cardiac enzyme levels in myocardial dysfunction in newborns with perinatal asphyxia. Indian J Pediatr. 2008;75:1223–1225. doi: 10.1007/s12098-008-0242-z. [DOI] [PubMed] [Google Scholar]
- 10.Suleiman MS, Lucchetti V, Caputo M, Angelini GD. Short periods of regional ischaemia and reperfusion provoke release of troponin I from the human hearts. Clin Chim Acta. 1999;284:25–30. doi: 10.1016/s0009-8981(99)00056-x. [DOI] [PubMed] [Google Scholar]
- 11.Türker G, Babaoğlu K, Gökalp AS, Sarper N, Zengin E, Arisoy AE. Cord blood cardiac troponin I as an early predictor of short-term outcome in perinatal hypoxia. Biol Neonate. 2004;86:131–137. doi: 10.1159/000079068. [DOI] [PubMed] [Google Scholar]
- 12.Thoresen M, Haaland K, Loberg EM, Whitelaw A, Apricena F, Hanko E, Steen PA. A piglet survival model of posthypoxic encephalopathy. Pediatr Res. 1996;40:738–748. doi: 10.1203/00006450-199611000-00014. [DOI] [PubMed] [Google Scholar]
- 13.Tooley JR, Satas S, Porter H, Silver IA, Thoresen M. Head cooling with mild systemic hypothermia in anesthetized piglets is neuroprotective. Ann Neurol. 2003;53:65–72. doi: 10.1002/ana.10402. [DOI] [PubMed] [Google Scholar]
- 14.Mount LE, Rowell JG. Body size, body temperature and age in relation to the metabolic rate of the pig in the first five weeks after birth. J Physiol. 1960;154:408–416. doi: 10.1113/jphysiol.1960.sp006587. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Tuchscherer M, Puppe B, Tuchscherer A, Tiemann U. Early identification of neonates at risk: traits of newborn piglets with respect to survival. Theriogenology. 2000;54:371–388. doi: 10.1016/S0093-691X(00)00355-1. [DOI] [PubMed] [Google Scholar]
- 16.Thoresen M, Satas S, Loberg EM, Whitelaw A, Acolet D, Lindgren C, Penrice J, Robertson N, Haug E, Steen PA. Twenty-four hours of mild hypothermia in unsedated newborn pigs starting after a severe global hypoxic-ischemic insult is not neuroprotective. Pediatr Res. 2001;50:405–411. doi: 10.1203/00006450-200109000-00017. [DOI] [PubMed] [Google Scholar]
- 17.Tooley J, Satas S, Eagle R, Silver IA, Thoresen M. Significant selective head cooling can be maintained long-term after global hypoxia ischemia in newborn piglets. Pediatrics. 2002;109:643–649. doi: 10.1542/peds.109.4.643. [DOI] [PubMed] [Google Scholar]
- 18.Andresen JH, Carlsen B, Solberg R, Morkrid L, Goverud IL, Loberg EM, Saugstad OD. Newborn piglets exposed to hypoxia after nicotine or saline pretreatment: long-term effects on brain and heart. J Matern Fetal Neonatal Med. 2009;22:161–168. doi: 10.1080/14767050802663186. [DOI] [PubMed] [Google Scholar]
- 19.Satas S, Loberg EM, Porter H, Whitelaw A, Steen PA, Thoresen M. Effect of global hypoxia-ischaemia followed by 24 h of mild hypothermia on organ pathology and biochemistry in a newborn pig survival model. Biol Neonate. 2003;83:146–156. doi: 10.1159/000067958. [DOI] [PubMed] [Google Scholar]
- 20.Campbell I. Chi-squared and Fisher-Irwin tests of two-by-two tables with small sample recommendations. Stat Med. 2007;26:3661–3675. doi: 10.1002/sim.2832. [DOI] [PubMed] [Google Scholar]
- 21.Edwards AD, Brocklehurst P, Gunn AJ, Halliday H, Juszczak E, Levene M, Strohm B, Thoresen M, Whitelaw A, Azzopardi D. Neurological outcomes at 18 months of age after moderate hypothermia for perinatal hypoxic ischaemic encephalopathy: synthesis and meta-analysis of trial data. BMJ. 2010;340:c363. doi: 10.1136/bmj.c363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Karlsson M, Tooley JR, Satas S, Hobbs CE, Chakkarapani E, Stone J, Porter H, Thoresen M. Delayed hypothermia as selective head cooling or whole body cooling does not protect brain or body in newborn pig subjected to hypoxia-ischemia. Pediatr Res. 2008;64:74–78. doi: 10.1203/PDR.0b013e318174efdd. [DOI] [PubMed] [Google Scholar]
- 23.Thoresen M, Simmonds M, Satas S, Tooley J, Silver IA. Effective selective head cooling during posthypoxic hypothermia in newborn piglets. Pediatr Res. 2001;49:594–599. doi: 10.1203/00006450-200104000-00024. [DOI] [PubMed] [Google Scholar]
- 24.Haaland K, Loberg EM, Steen PA, Thoresen M. Posthypoxic hypothermia in newborn piglets. Pediatr Res. 1997;41:505–512. doi: 10.1203/00006450-199704000-00009. [DOI] [PubMed] [Google Scholar]
- 25.National Institute for Health and Clinical Excellence [Accessed, June 13, 2011];Therapeutic hypothermia with intracorporeal temperature monitoring for hypoxic perinatal brain injury. 2010 Available at: http://www.nice.org.uk/nicemedia/live/11315/48809/48809.pdf.
- 26.Polderman KH. Induced hypothermia and fever control for prevention and treatment of neurological injuries. Lancet. 2008;371:1955–1969. doi: 10.1016/S0140-6736(08)60837-5. [DOI] [PubMed] [Google Scholar]
- 27.Gressens P, Dingley J, Plaisant F, Porter H, Schwendimann L, Verney C, Tooley J, Thoresen M. Analysis of neuronal, glial, endothelial, axonal and apoptotic markers following moderate therapeutic hypothermia and anesthesia in the developing piglet brain. Brain Pathol. 2008;18:10–20. doi: 10.1111/j.1750-3639.2007.00095.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Panteghini M, Bonora R, Pagani F, Buffoli F, Cuccia C. Rapid, highly sensitive immunoassay for determination of cardiac troponin I in patients with myocardial cell damage. Clin Chem. 1997;43:1464–1465. [PubMed] [Google Scholar]
- 29.Hunkeler NM, Kullman J, Murphy AM. Troponin I isoform expression in human heart. Circ Res. 1991;69:1409–1414. doi: 10.1161/01.res.69.5.1409. [DOI] [PubMed] [Google Scholar]
- 30.Bertsch T, Janke C, Denz C, Weiss M, Luiz T, Ellinger K, Korth U, Hannak D, Bartelt U, Krieter H. Cardiac troponin I and cardiac troponin T increases in pigs during ischemia-reperfusion damage. Exp Toxicol Pathol. 2000;52:157–159. doi: 10.1016/S0940-2993(00)80111-6. [DOI] [PubMed] [Google Scholar]
- 31.York M, Scudamore C, Brady S, Chen C, Wilson S, Curtis M, Evans G, Griffiths W, Whayman M, Williams T, Turton J. Characterization of troponin responses in isoproterenol-induced cardiac injury in the Hanover Wistar rat. Toxicol Pathol. 2007;35:606–617. doi: 10.1080/01926230701389316. [DOI] [PubMed] [Google Scholar]
- 32.Taggart DP, Hadjinikolas L, Hooper J, Albert J, Kemp M, Hue D, Yacoub M, Lincoln JC. Effects of age and ischemic times on biochemical evidence of myocardial injury after pediatric cardiac operations. J Thorac Cardiovasc Surg. 1997;113:728–735. doi: 10.1016/S0022-5223(97)70231-9. [DOI] [PubMed] [Google Scholar]
- 33.Zhou WH, Shao XM, Zhang XD, Chen C, Huang GY. [Effects of hypothermia on cardiac function in neonates with asphyxia] Zhonghua Er Ke Za Zhi. 2003;41:460–462. [PubMed] [Google Scholar]
- 34.Mavroudis C, Backer CL. Pediatric Cardiac Surgery. Mosby, Philadephia: 2003. pp. 39–46. [Google Scholar]
- 35.Donnelly WH, Bucciarelli RL, Nelson RM. Ischemic papillary muscle necrosis in stressed newborn infants. J Pediatr. 1980;96:295–300. doi: 10.1016/s0022-3476(80)80833-x. [DOI] [PubMed] [Google Scholar]
- 36.Chakkarapani E, Dingley J, Liu X, Hoque N, Aquilina K, Porter H, Thoresen M. Xenon enhances hypothermic neuroprotection in asphyxiated newborn pigs. Ann Neurol. 2010;68:330–341. doi: 10.1002/ana.22016. [DOI] [PubMed] [Google Scholar]