

Abstract
Bacille Calmette-Guerin (BCG) has been used extensively as a vaccine against human tuberculosis. Herein, we describe gluteal tuberculosis abscess due to inadvertently injected BCG a patient with bladder cancer.
Keywords: Bacille Calmette-Guerin, bladder cancer, gluteal abscess, tuberculosis
Bacille Calmette–Guérin (BCG) has been used extensively as a vaccine against human tuberculosis for over 70 years. In addition to its role as a vaccine against tuberculosis, BCG has also been used as an immunotherapeutic agent by intravesical instillation in superficial cancer of the bladder.[1–3] Side effects and complications of such immunotherapy are usually local, self-limited and minor in nature, but occasionally it may result in severe and systemic manifestations.[2,3]
Herein, we report a gluteal tuberculosis abscess as a consequence of inadvertently injected BCG to a patient with bladder cancer.
Case Report
A 51-year-old man was recommended to have six doses of intravesical BCG instillation for a superficial bladder cancer. BCG was erroneously injected intramuscularly for four weeks. Patient's vital signs at admission were as follows: Temperature 38.8°C, pulse 96/min, respiratory rate 16/min, and blood pressure 132/85 mmHg. On physical examination right gluteal swelling, erythema, tenderness, and indurations were detected. The physical examination findings were unremarkable for other systems. The patient had no other co-morbid disease except type II DM. Ultrasonographic evaluations revealed a hypoechoic loculation compatible with gluteal abscess [Figure 1]. Chest radiography and computed tomography did not reveal any active or old TB lesion [Figures 2 and 3]. Tuberculin skin test was negative after 72 h. Abscess microscopy and cultures for acid fast bacilli (AFP) were positive without any other microorganisms. Pyrazinamide-resistant Mycobacterium tuberculosis complex was isolated. Sputum cultures were negative for mycobacterium. With these findings antituberculosis treatment (Rifampicin, Isoniazid, Ethambutol and Ciprofloxacin) was started together with incision and drainage of abscess. Patient responded well to these treatment and nine months later the patient was fully recovered from the disease.
Figure 1.
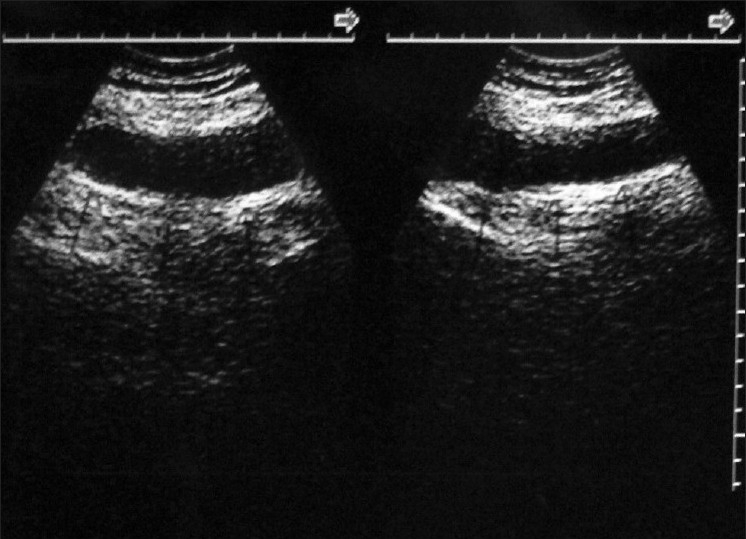
Ultrasonography reveals a well-defined hypoechoic homogeneous mass 10 × 8 cm in diameter
Figure 2.
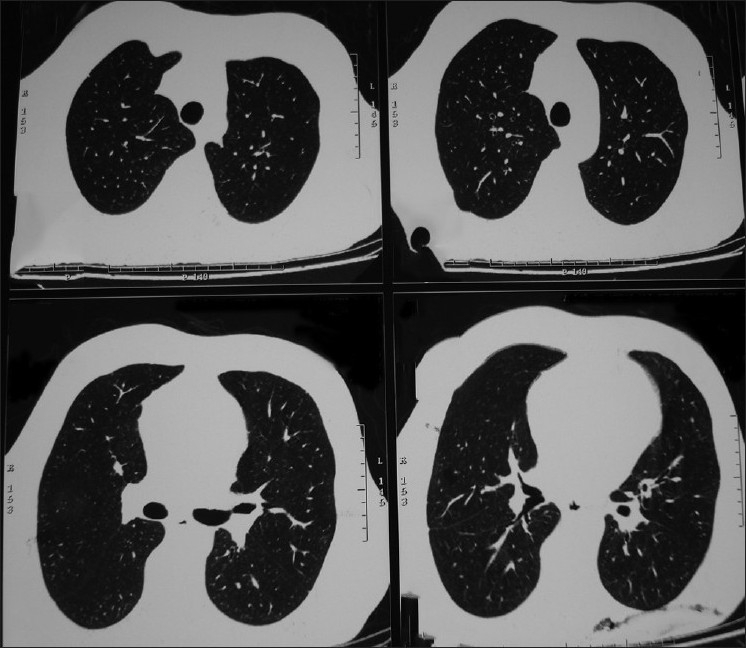
Chest CT scan showing the emphysematous changes
Figure 3.
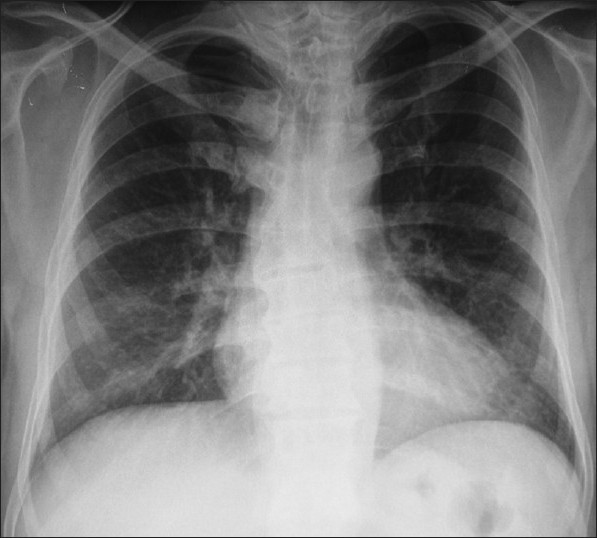
There is no active or old lesion of TB in chest X-ray
Discussion
Adverse reactions to BCG vaccination can be categorized into two major categories: Non-infectious and infectious. Most of the reported complications are abnormal primary complexes, either lesions at the injection site or, more commonly, suppurative lymphadenitis. Lesions at the injection site were ulcers, subcutaneous abscesses, or necrotic lesions due to excessive delayed hypersensitivity reactions. Other complications were localized or generalized non-fatal persisting BCG infection, and fatal disseminated BCG infection.[4,5]
Intramuscular administration of BCG is rare and usually due to an error in the administration. Only a few cases are reported in the literature.[6,7] The previously reported gluteal tuberculosis cases were not confirmed bacteriologically and treated empirically.[8] But it is necessary to obtain aspirated pus from abscesses at the site of immunization to confirm that BCG is the cause or to identify other organisms that occasionally cause such reactions. In the presented case aspirated pus was obtained and gluteal tuberculosis was proven by abscess microscopy and cultures. No other microorganisms were seen on abscess microscopy and cultures.
Various interventions including; drainage, needle aspiration, topical or systemic isoniazid, or systemic erythromycin, have been used for post-injection ulcers and abscesses due to BCG.[2,3] Mycobacterium bovis including BCG are known to be naturally resistant to PZA and these features are commonly used to distinguish M. bovis from M. tuberculosis.[9] The natural Pyrazinamide resistance in M. bovis and BCG is due to a single point mutation of pncA gene.[10] Because of these reasons Pyrazinamide was not used. The present case was treated with daily doses of Rifampicin, Izoniazid, Ethambutol and Ciprofloxacin due to persistent fever.
In conclusion, this case report shows that specific treatment is an invaluable conjunct to drainage in patients with abscess secondary to inadvertently injected BCG. But the most important thing is to prevent such undesired complications by adequate training of the health personnel and patients.
Footnotes
Source of Support: Nil,
Conflict of Interest: None declared.
References
- 1.Krege S, Giani G, Meyer R, Otto T, Rubben H. A randomized multicenter trial of adjuvant therapy in superficial bladder cancer: Transurethral resection plus bacillus Calmette-Guérin. J Urol. 1996;156:962–6. doi: 10.1016/s0022-5347(01)65673-8. [DOI] [PubMed] [Google Scholar]
- 2.Lamm DL. Complications of bacillus Calmette-Guérin immunotherapy. Urol Clin North Am. 1992;19:565–72. [PubMed] [Google Scholar]
- 3.Grange JM. Complications of bacille Calmette-Guerin (BCG) vaccination and immunotherapy and their management. Commun Dis Publ Health. 1998;1:84–8. [PubMed] [Google Scholar]
- 4.Lotte A, Wasz-Höckert O, Poisson N, Dumitrescu N, Verron M, Couvet E. BCG complications. Adv Tuberc Res. 1984;21:107–93. [PubMed] [Google Scholar]
- 5.de Souza GR, Sant’Anna CC, Lapa e Silva JR, Mano DB, Bethlem NM. Intradermal BCG vaccination complications - analysis of 51 cases. Tubercle. 1983;64:23–7. doi: 10.1016/0041-3879(83)90046-6. [DOI] [PubMed] [Google Scholar]
- 6.Kulkarni AG, Kulkarni SA. Primary intramuscular cold abscess in the left deltoid region. East Afr Med J. 1990;67:922–33. [PubMed] [Google Scholar]
- 7.Pasteur MC, Hall DR. The effects of inadvertent intramuscular injection of BCG vaccine. Scand J Infect Dis. 2001;33:473–4. doi: 10.1080/00365540152029981. [DOI] [PubMed] [Google Scholar]
- 8.Yarmohammadi A, Ahmadinia H, Abolbashari M, Molaei M. Results of inadvertent administration of bacillus Calmette-Guerin for treatment of transitional cell carcinoma of bladder. Urol J. 2007;4:121–2. [PubMed] [Google Scholar]
- 9.de Jong BC, Onipede A, Pym AS, Gagneux S, Aga RS, DeRiemer K, et al. Does resistance to pyrazinamide accurately indicate the presence of Mycobacterium bovis? J Clin Microbiol. 2005;43:3530–2. doi: 10.1128/JCM.43.7.3530-3532.2005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Scorpio A, Zhang Y. Mutations in pncA, a gene encoding pyrazinamidase/nicotinamidase, cause resistance to the antituberculous drug pyrazinamide in tubercle bacillus. Nat Med. 1996;2:662–7. doi: 10.1038/nm0696-662. [DOI] [PubMed] [Google Scholar]