

Abstract
Objective. The aim of this study is to develop a prognostic model capable of predicting the probability of significant upgrading among Japanese patients. Methods. The study cohort comprised 508 men treated with RP, with available prostate-specific antigen levels, biopsy, and RP Gleason sum values. Clinical and pathological data from 258 patients were obtained from another Japanese institution for validation. Results. Significant Gleason sum upgrading was recorded in 92 patients (18.1%) at RP. The accuracy of the nomogram predicting the probability of significant Gleason sum upgrading between biopsy and RP specimens was 88.9%. Overall AUC was 0.872 when applied to the validation data set. Nomogram predictions of significant upgrading were within 7.5% of an ideal nomogram. Conclusions. Nearly one-fifth of Japanese patients with prostate cancer will be significantly upgraded. Our nomogram seems to provide considerably accurate predictions regardless of minor variations in pathological assessment when applied to Japanese patient populations.
1. Introduction
Pretreatment prostate-specific antigen (PSA) level, Gleason score, and pathological stage are generally recognized as significant predictors of biochemical recurrence in patients with clinically localized prostate cancer treated by radical prostatectomy (RP) [1]. A finding of high-grade disease in RP specimens is an adverse prognostic factor, and such tumors are significantly more likely to progress than organ-confined cancers. In addition, this finding is associated with a greater risk of positive surgical margins, further decreasing the likelihood of long-term cancer control. Determining whether a patient has high-grade disease is thus important for treatment selection and prognosis [2].
Chun et al. developed and validated a model predicting Gleason sum upgrading from biopsy to final pathology using clinical variables (PSA level, clinical stage, and biopsy Gleason sum) [3]. That model relies on three readily available clinical variables, all of which are significant uni- and multivariate predictors of biopsy Gleason sum upgrading. Based on the importance of the concept of Gleason sum upgrading in decision making for prostate cancer, we previously performed a formal external validation using a fully independent data set in a contemporary cohort of two Japanese institutions [4]. Unfortunately, our results did not suggest that accurate predictions may be expected when using this nomogram across different racial patient populations. Development of a nomogram predicting the probability of biopsy Gleason sum upgrading in a large multi-institutional cohort among Japanese patients thus appears essential.
2. Material and Methods
Clinical and pathological data were prospectively gathered from 837 consecutive patients at two centers (Department of Urology in the Graduate School of Medicine at Chiba University, Chiba (n = 327) and Division of Urology at Chiba Cancer Center, Chiba (n = 510)). Of these, 71 patients were excluded because of missing data.
Analyses targeted 766 evaluable patients assessed with ≥10 biopsy cores. All men had biopsy-confirmed, clinically localized prostate cancer, and all underwent RP between January 2003 and December 2009. Patients treated with neoadjuvant hormonal therapy were excluded, as the nomogram is not applicable in these men.
Clinical stage was assigned by the attending urologist according to the 2002 TNM system. Under transrectal ultrasound (TRUS) guidance, 10–16 needle cores were obtained. Pretreatment PSA levels were measured before a digital rectal examination (DRE) and TRUS. Biopsy Gleason sum was assigned by pathologists from each center. All RP specimens were processed according to the Stanford protocol and graded according to the Gleason system [5].
Significant upgrading was defined as a biopsy Gleason sum changing from ≤6 to ≥7 or from 7 to ≥8, according to previous reports by King [6] and King and Long [7]. For both patient cohorts, the same predictors, that is, PSA level, primary and secondary biopsy Gleason score, and clinical stage, were used in uni- and multivariate logistic regression models addressing the rate of significant Gleason sum upgrading between biopsy and RP pathology. Coefficients of multivariate logistic regression models were then used to develop a nomogram predicting the probability of significant Gleason sum upgrading, using the data from one Japanese institution: the Division of Urology at Chiba Cancer Center, Chiba (n = 508). The variables were selected for the final multivariate model by forward stepwise selection. In addition, we utilized the bootstrapping method to correct for overfit and the bias-corrected coefficients obtained from multivariate analysis to construct the final nomogram. Accuracy of the nomogram was quantified using the receiver operating characteristics (ROC) curve.
Validation data representing men treated with RP were obtained from another Japanese institution: the Department of Urology in the Graduate School of Medicine at Chiba University, Chiba (n = 258). To determine the nomogram-predicted probability of significant Gleason sum upgrading, we applied the nomogram (Figure 1) to all 258 observations. Accuracy of the nomogram was then quantified using the area under the curve (AUC) for external validation. The extent of over- or underestimation relative to the observed rate of significant upgrading was explored graphically using nonparametric Loess smoothing plots. All tests were two sided with a significance level set at P < .05.
Figure 1.
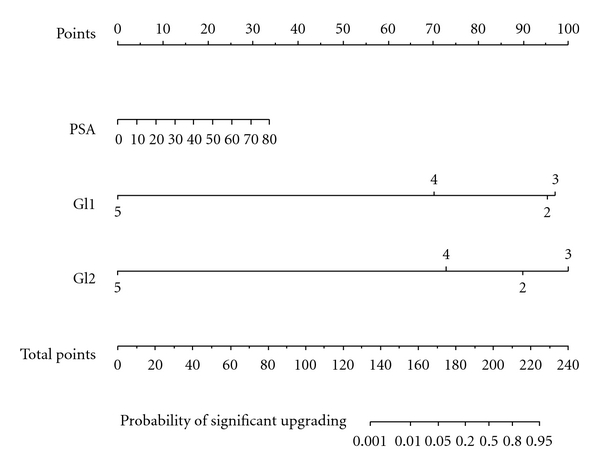
Nomogram based on 508 patients treated at Chiba Cancer Center, for predicting significant Gleason sum upgrading between biopsy and radical prostatectomy. PSA: prostate-specific antigen (ng/mL); Gl1: primary biopsy Gleason score; Gl2: secondary biopsy Gleason score. To obtain the nomogram-predicted probability of significant biopsy upgrading, locate the patient values at each axis, draw a vertical line to the “Points” axis to determine how many points are attributed to each variable value; total the points for all variables, and locate the sum on the “Total Points” line to assess the individual probability of significant biopsy Gleason sum upgrading on the Probability of Significant Upgrading line.
3. Results
Table 1 lists the clinical and pathological characteristics of patients included in this study, and data were stratified for participating institutions. Pretreatment PSA levels were 2.5–79.7 ng/mL. Clinical stages T1c and T2 were recorded in 685 patients (89.4%). Among all men, 578 (75.5%) showed a biopsy Gleason sum of 6 or 7.
Table 1.
Descriptive characteristics of subgroups according to institutions.
| Variable | Chiba Cancer Center | Chiba University | |
|---|---|---|---|
| n | 508 | 258 | |
| Age (years) | Mean | 66.902 | 65.054 |
| SD | 4.975 | 5.253 | |
| Median | 67 | 65 | |
| Min | 52 | 49 | |
| Max | 78 | 76 | |
|
| |||
| PSA (ng/mL) | Mean | 13.977 | 11.616 |
| SD | 12.194 | 9.732 | |
| Median | 9.755 | 8.420 | |
| Min | 2.588 | 2.450 | |
| Max | 79.710 | 72.000 | |
|
| |||
| Clinical stage (%) | T1c | 169 (33.3) | 180 (69.8) |
| T2a | 172 (33.9) | 32 (12.4) | |
| T2b | 89 (17.5) | 15 (5.8) | |
| T2c | 12 (2.4) | 16 (6.2) | |
| T3 | 66 (13.0) | 15 (5.8) | |
|
| |||
| Biopsy Gleason primary (%) | ≤3 | 318 (62.6) | 172 (66.7) |
| 4 | 167 (32.9) | 80 (31.0) | |
| 5 | 23 (4.5) | 6(2.3) | |
|
| |||
| Biopsy Gleason secondary (%) | ≤3 | 197 (38.8) | 128 (49.6) |
| 4 | 227 (44.7) | 112 (43.4) | |
| 5 | 84 (16.5) | 18 (7.0) | |
|
| |||
| Biopsy Gleason sum (%) | ≤6 | 123 (24.2) | 91 (35.3) |
| 7 | 248 (48.8) | 116 (45.0) | |
| 8 | 58 (11.4) | 31 (12.0) | |
| 9 | 74 (14.6) | 18 (7.0) | |
| 10 | 5 (1.0) | 2 (0.8) | |
|
| |||
| Pathological Gleason primary (%) | ≤3 | 327 (64.4) | 151 (58.5) |
| 4 | 155 (30.5) | 104 (40.3) | |
| 5 | 26 (5.1) | 3 (1.2) | |
|
| |||
| Pathological Gleason secondary (%) | ≤3 | 209 (41.1) | 114 (44.2) |
| 4 | 241 (47.4) | 119 (46.1) | |
| 5 | 58 (11.4) | 25 (9.7) | |
|
| |||
| Pathological Gleason sum (%) | ≤6 | 93 (18.3) | 44 (17.1) |
| 7 | 332 (65.4) | 176 (68.2) | |
| 8 | 21 (4.1) | 11 (4.3) | |
| 9 | 60 (11.8) | 27 (10.5) | |
| 10 | 2 (0.4) | 0 (0.0) | |
|
| |||
| Significant upgrading Gleason sum (%) | 92 (18.1) | 64 (24.8) | |
In the Chiba Cancer Center dataset (508 men), concordance between biopsy and RP Gleason sum was recorded in 258 (50.8%). Upgrading was recorded in 104 men (20.5%), whereas 146 (28.7%) were downgraded. These data also indicate that 69 patients (13.6%) were upgraded from biopsy Gleason sum ≤6 to pathologic Gleason sum ≥7. The rate of upgrading from biopsy Gleason sum 7 to pathologic Gleason sum ≥8 was 4.5% (n = 23). The overall rate of significant upgrading from biopsy to pathologic Gleason sum was 18.1% (92 patients). Conversely, Gleason sum decreased from ≥8 to ≤7 in 82 men (16.1%) and from 7 to ≤6 in 36 (7.1%). Stratified according to institutions, agreement between Gleason biopsy and final pathology was more frequent in the Chiba University data set (146 men, 56.6%) than in that from Chiba Cancer Center (50.8%). Significant upgrading was more frequent for Chiba University (64 men, 24.8%) than for Chiba Cancer Center (92, 18.1%). We also investigated temporal changes in the rate of significant Gleason sum upgrading for two institutions. Although no significant correlation was found, a trend toward a decrease in the rate of significant upgrading since 2006 was seen.
Table 2 shows uni- and multivariate logistic regression models for PSA, clinical stage, and primary and secondary biopsy Gleason scores with corresponding uni- and multivariate predictive accuracy estimates. Clinical stage was not associated with significant upgrading in univariate analysis (P = .131) and was excluded for multivariate analyses. In univariate analyses, primary and secondary biopsy Gleason scores were highly significant predictors of significant Gleason sum upgrading (P < .001 and P = .002, resp.). Of all predictors, secondary biopsy Gleason score (AUC = 0.784) represented the most informative predictor, followed by primary biopsy Gleason score (AUC = 0.712) and PSA (AUC = 0.569). In multivariate analyses, all variables except for clinical stage were highly significant (P ≤ .001). Multivariate 200 bootstrap-corrected predictive accuracy was 88.9% and exceeded the most informative univariate predictor, namely secondary biopsy Gleason score (78.4%). Figure 1 shows the regression coefficient-based nomogram. High PSA values as well as low primary and/or secondary biopsy Gleason scores are risk factors for significant Gleason sum upgrading at final pathology.
Table 2.
Uni- and multivariate logistic regression models predicting significant Gleason sum upgrading.
| Predictors | Univariate predictive | Univariate model | Multivariate model | ||
|---|---|---|---|---|---|
| accuracy | OR | P | OR | P | |
| Preoperative PSA | 0.569 | 1.020 | .025 | 1.047 | <.001 |
| Clinical stage | NA | ||||
| 1c | 1.000 | ||||
| 2a | 0.978 | .934 | NA | NA | |
| 2b | 0.715 | .334 | NA | NA | |
| 2c | 0.000 | .983 | NA | NA | |
| 3 | 0.528 | .131 | NA | NA | |
| Biopsy Gleason primary | 0.712 | ||||
| 2 | 1.000 | ||||
| 3 | 0.250 | <.001 | 1.210 | .677 | |
| 4 | 0.041 | <.001 | 0.064 | <.001 | |
| 5 | 0.000 | .983 | 0.000 | .992 | |
| Biopsy Gleason secondary | 0.784 | ||||
| 2 | 1.000 | ||||
| 3 | 1.491 | .435 | 3.050 | .041 | |
| 4 | 0.189 | .002 | 0.156 | .001 | |
| 5 | 0.000 | .98 | 0.000 | .986 | |
| Predictive accuracy | 0.889 | ||||
OR: odds ratio; PSA: prostate-specific antigen; NA: not assessed.
Figure 2 illustrates how predictions of the nomogram are compared with actual probabilities for the validation data (258 men). The x-axis represents nomogram predictions, and the y-axis represents the observed rate of significant Gleason upgrading for patients in the validation cohort. Accuracy of the nomogram was 87.2% (confidence interval, 82.7–91.7%). The dashed 45° line represents the performance of an ideal nomogram, where predicted outcome would correspond perfectly with actual outcome. The performance of our nomogram is plotted as the solid line. The dotted lines represent a 7.5% margin of error, and the nomogram calibration plot demonstrated virtually ideal predictions. The rate of predicted significant Gleason upgrading closely paralleled the observed rate of Gleason upgrading, nearly corresponding to the 45° line and always within the 7.5% margin of error. The correspondence seen between actual and ideal nomogram predictions suggests good calibration of the nomogram in the validation cohort.
Figure 2.
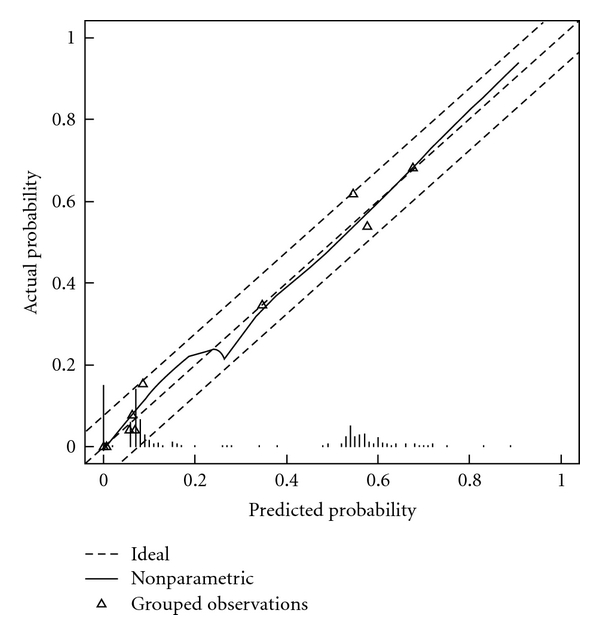
Calibration plot for external validation cohort. The x-axis shows the prediction calculated using the nomogram, and the y-axis gives observed rates of significant Gleason sum upgrading for patients in the validation cohort. Dashed line indicates reference line, where an ideal nomogram would lie. Solid line indicates performance of the nomogram applied to the validation cohort. The solid line is close to the dashed line of the ideal nomogram and is always within the 7.5% margin of error.
4. Discussion
Biopsy upgrading has important clinical implications in terms of watchful waiting, surgery, and radiotherapy (RT) candidates [8–10]. Most reported biopsy Gleason sums are either 6 or 7, and these Gleason sums are at greatest risk of being upgraded. However, tools have previously been unavailable for reliably and accurately predicting this phenomenon. Previous reports have indicated that with more extended biopsy schemes, the risk of upgrading decreases [8, 11] due to higher sampling density and more accurate evaluation of the pathological biopsy. Extended biopsy schemes (≥10 cores) might affect the rate of and ability to predict biopsy Gleason sum upgrading [12]. As a result, ≥14 needle cores are currently obtained in our institutions [13].
King [6] and King and Long [7] defined significant Gleason sum upgrading as a Gleason sum increase either from ≤6 to ≥7 or from 7 to ≥8 between biopsy and RP specimens. They distinguished between any upgrading and significant upgrading and suggested that significant upgrading represents a clinically meaningful entity. Predicting the rate of significant upgrading would be much more clinically meaningful, since these three categories represent pathologically and clinically different diseases. A preparative nomogram predicting the probability of significant Gleason sum upgrading was developed among Western populations [14]. Given the utility of the concept, creation of a new prediction tool based on a modern, Japanese-only cohort and aimed at predicting significant upgrading represents a worthwhile goal.
These findings are important as a first substantial depiction of the rate of significant Gleason sum upgrading in a Japanese contemporary cohort. Several applications of these findings can be considered. For example, the choice of interstitial brachytherapy might be reconsidered in men who are at greater risk of biopsy Gleason sum upgrading. Similarly, neoadjuvant hormonal therapy might be considered if radiotherapy is contemplated. Finally, among surgical candidates, the risk of significant Gleason sum upgrading might contribute to different considerations regarding the extent of neurovascular bundle resection and the implications of positive surgical margins. However, the decision of what level of risk is required for more aggressive therapy remains controversial.
Chun et al. indicated that the rate of upgrading decreased over time [3]. We also investigated temporal changes in the rate of significant Gleason sum upgrading and found no significance. However, a trend toward a decreased rate of significant upgrading over time since 2006 was apparent. This decrease may be due to the impact of the 2005 International Society of Urological Pathology (ISUP) modified Gleason grading system [15]. A shift towards a higher Gleason sum on biopsy might also have occurred after the ISUP consensus [16].
Prostate cancer is one of the most common cancers among Western populations, and incidence is increasing in Asia, although considerable differences in incidence and biological aggressiveness remain between Western and Asian populations [17]. Epidemiological and genetic differences in prostate cancers exist between patients in Japan and the United States, and p53 gene mutational analysis, which often provides information about etiological factors, has revealed clear differences in p53 gene mutational spectra between Japanese and Western cases [18]. Differences in hormone levels in various racial/ethnic groups have been suggested to account for part of the differences in prostate cancer risk. Racial/ethnic differences in the intraprostatic testosterone/dihydrotestosterone conversion ratio would provide important support for the hypothesis that differences in the enzymatic activity of 5a-reductase within the prostate gland can explain most of the racial/ethnic differences in prostate cancer risk [19–21].
We have previously performed a formal external validation of a preparative nomogram predicting the probability of Gleason sum upgrading developed among Western populations, using a fully independent data set in a contemporary cohort of two Japanese institutions [4]. The nomogram provided reasonably accurate predictions regardless of minor variations in pathological assessment but could not necessarily be considered accurate when applied to Japanese patient populations. Our previous results suggested that development of a nomogram predicting the probability of biopsy Gleason sum upgrading in a large multi-institutional cohort among Japanese patients is essential.
We are the first to develop multivariate models to predict significant Gleason sum upgrading between biopsy and RP in Japanese populations. Our current model was 88.9% accurate in predicting the probability of significant Gleason sum upgrading. To date, no other models capable of accurately predicting the rate of significant upgrading are available for Japanese patients. Consequently, this model represents the only alternative to clinical ratings of the probability of significant Gleason sum upgrading. We have therefore tested the performance of the nomogram in an external validation dataset, and overall AUC was 0.87. Individual treatment centers in this study differed with respect to patient selection, extracapsular extension measurement, and follow up assessment. Furthermore, no centralized review of pathology was performed. For the purposes of nomogram validation, such heterogeneity is desirable to gain insights into how the nomogram will perform across varied settings [22]. The nomogram was consistently accurate at both centers, with AUC ranging from 0.87 to 0.89. Our nomogram thus seems to provide reasonably accurate predictions regardless of minor variations in pathological assessment.
Clear limitations exist to this study. We included 10–16 core biopsy data in the cohort, but the difference in rate of upgrading was not significant between these biopsy regimens according to the current data [14]. However, biopsy schemes that rely on taking even more cores might be associated with a lower rate of biopsy Gleason sum upgrading [23–25]. In addition to the small population size, the level of experience of pathologists could also affect the findings. Finally, model accuracy could potentially be improved by integrating additional predictor variables, for example, the level of expertise of the pathologist, or existing biomarkers [26]. If the ISUP modified Gleason grading system or central pathology diagnosis system was introduced, this nomogram should be more useful for daily clinical practice. Despite these limitations, our model represents an important contribution concerning the rate of significant Gleason sum upgrading between biopsy and final pathology.
5. Conclusions
Significant Gleason sum upgrading between biopsy and final pathology represents an important consideration in treatment decision making, even in most contemporary patients. Our nomogram was 88.9% accurate in predicting the probability of significant Gleason sum upgrading, and seems to provide accurate predictions regardless of minor variations in pathological assessment when applied to Japanese patient populations.
Acknowledgments
This work was supported by Grants-in-Aid from the Ministry of Education, Culture, Sports, Science and Technology of Japan (contract Grant no. 21791488), the Japanese Foundation for Prostate Research (2004), the Japanese Urological Association (2006), and the Yamaguchi Endocrine Research Association.
Abbreviations and Acronyms
- RP:
Radical prostatectomy
- AUC:
Area under the receiver operating characteristic curve
- PSA:
Prostate-specific antigen
- TRUS:
Transrectal ultrasound
- DRE:
Digital rectal examination
- ROC:
Receiver operating characteristics
- RT:
Radiotherapy
- ISUP:
International Society of Urological Pathology.
References
- 1.Imamoto T, Suzuki H, Fukasawa S, et al. Pretreatment serum testosterone level as a predictive factor of pathological stage in localized prostate cancer patients treated with radical prostatectomy. European Urology. 2005;47(3):308–312. doi: 10.1016/j.eururo.2004.11.003. [DOI] [PubMed] [Google Scholar]
- 2.Yano M, Imamoto T, Suzuki H, et al. The clinical potential of pretreatment serum testosterone level to improve the efficiency of prostate cancer screening. European Urology. 2007;51(2):375–380. doi: 10.1016/j.eururo.2006.08.047. [DOI] [PubMed] [Google Scholar]
- 3.Chun FK-H, Steuber T, Erbersdobler A, et al. Development and internal validation of a nomogram predicting the probability of prostate cancer Gleason sum upgrading between biopsy and radical prostatectomy pathology. European Urology. 2006;49(5):820–826. doi: 10.1016/j.eururo.2005.11.007. [DOI] [PubMed] [Google Scholar]
- 4.Imamoto T, Suzuki H, Utsumi T, et al. External validation of a nomogram predicting the probability of prostate cancer gleason sum upgrading between biopsy and radical prostatectomy pathology among Japanese patients. Urology. 2010;76(2):404–410. doi: 10.1016/j.urology.2009.05.084. [DOI] [PubMed] [Google Scholar]
- 5.Aus G, Abbou CC, Bolla M, et al. EAU guidelines on prostate cancer. European Urology. 2005;48(4):546–551. doi: 10.1016/j.eururo.2005.06.001. [DOI] [PubMed] [Google Scholar]
- 6.King CR. Patterns of prostate cancer biopsy grading: trends and clinical implications. International Journal of Cancer. 2000;90(6):305–311. doi: 10.1002/1097-0215(20001220)90:6<305::aid-ijc1>3.0.co;2-u. [DOI] [PubMed] [Google Scholar]
- 7.King CR, Long JP. Prostate biopsy grading errors: a sampling problem? International Journal of Cancer. 2000;90(6):326–330. doi: 10.1002/1097-0215(20001220)90:6<326::aid-ijc3>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 8.King CR, McNeal JE, Gill H, Presti JC., Jr. Extended prostate biopsy scheme improves reliability of Gleason grading: implications for radiotherapy patients. International Journal of Radiation Oncology Biology Physics. 2004;59(2):386–391. doi: 10.1016/j.ijrobp.2003.10.014. [DOI] [PubMed] [Google Scholar]
- 9.Kulkarni GS, Lockwood G, Evans A, et al. Clinical predictors of gleason score upgrading: implications for patients considering watchful waiting, active surveillance, or brachytherapy. Cancer. 2007;109(12):2432–2438. doi: 10.1002/cncr.22712. [DOI] [PubMed] [Google Scholar]
- 10.Roemeling S, Roobol MJ, de Vries SH, et al. Active surveillance for prostate cancers detected in three subsequent rounds of a screening trial: characteristics, PSA doubling times, and outcome. European Urology. 2007;51(5):1244–1251. doi: 10.1016/j.eururo.2006.11.053. [DOI] [PubMed] [Google Scholar]
- 11.King CR, Patel DA, Terris MK. Prostate biopsy volume indices do not predict for significant gleason upgrading. American Journal of Clinical Oncology. 2005;28(2):125–129. doi: 10.1097/01.coc.0000143848.24158.c3. [DOI] [PubMed] [Google Scholar]
- 12.Capitanio U, Karakiewicz PI, Jeldres C, et al. The probability of Gleason score upgrading between biopsy and radical prostatectomy can be accurately predicted. International Journal of Urology. 2009;16(5):526–529. doi: 10.1111/j.1442-2042.2009.02270.x. [DOI] [PubMed] [Google Scholar]
- 13.Inahara M, Suzuki H, Kojima S, et al. Improved prostate cancer detection using systematic 14-core biopsy for large prostate glands with normal digital rectal examination findings. Urology. 2006;68(4):815–819. doi: 10.1016/j.urology.2006.05.010. [DOI] [PubMed] [Google Scholar]
- 14.Chun FK-H, Briganti A, Shariat SF, et al. Significant upgrading affects a third of men diagnosed with prostate cancer: predictive nomogram and internal validation. BJU International. 2006;98(2):329–334. doi: 10.1111/j.1464-410X.2006.06262.x. [DOI] [PubMed] [Google Scholar]
- 15.Epstein JI, Allsbrook WC, Jr., Amin MB, et al. The 2005 International Society of Urological Pathology (ISUP) consensus conference on Gleason grading of prostatic carcinoma. American Journal of Surgical Pathology. 2005;29(9):1228–1242. doi: 10.1097/01.pas.0000173646.99337.b1. [DOI] [PubMed] [Google Scholar]
- 16.Zareba P, Zhang J, Yilmaz A, Trpkov K. The impact of the 2005 International Society of Urological Pathology (ISUP) consensus on Gleason grading in contemporary practice. Histopathology. 2009;55(4):384–391. doi: 10.1111/j.1365-2559.2009.03405.x. [DOI] [PubMed] [Google Scholar]
- 17.Imamoto T, Suzuki H, Yano M, et al. The role of testosterone in the pathogenesis of prostate cancer. International Journal of Urology. 2008;15(6):472–480. doi: 10.1111/j.1442-2042.2008.02074.x. [DOI] [PubMed] [Google Scholar]
- 18.Suzuki H, Komiya A, Aida S, Ito H, Yatani R, Shimazaki J. Detection of human papillomavirus DNA and p53 gene mutations in human prostate cancer. Prostate. 1996;28(5):318–324. doi: 10.1002/(SICI)1097-0045(199605)28:5<318::AID-PROS8>3.0.CO;2-7. [DOI] [PubMed] [Google Scholar]
- 19.Ross RK, Pike MC, Coetzee GA, et al. Androgen metabolism and prostate cancer: establishing a model of genetic susceptibility. Cancer Research. 1998;58(20):4497–4504. [PubMed] [Google Scholar]
- 20.Imamoto T, Suzuki H, Yano M, et al. Does presence of prostate cancer affect serum testosterone levels in clinically localized prostate cancer patients? Prostate Cancer and Prostatic Diseases. 2009;12(1):78–82. doi: 10.1038/pcan.2008.35. [DOI] [PubMed] [Google Scholar]
- 21.Ross RK, Bernstein L, Lobo RA, et al. 5-alpha-reductase activity and risk of prostate cancer among Japanese and US white and black males. Lancet. 1992;339(8798):887–889. doi: 10.1016/0140-6736(92)90927-u. [DOI] [PubMed] [Google Scholar]
- 22.Suzuki H, Komiya A, Kamiya N, et al. Development of a nomogram to predict probability of positive initial prostate biopsy among Japanese patients. Urology. 2006;67(1):131–136. doi: 10.1016/j.urology.2005.07.040. [DOI] [PubMed] [Google Scholar]
- 23.Moussa AS, Kattan MW, Berglund R, Yu C, Fareed K, Jones JS. A nomogram for predicting upgrading in patients with low-and intermediate-grade prostate cancer in the era of extended prostate sampling. BJU International. 2010;105(3):352–358. doi: 10.1111/j.1464-410X.2009.08778.x. [DOI] [PubMed] [Google Scholar]
- 24.Ohigashi T, Kanao K, Mizuno R, Kikuchi E, Nakashima J, Oya M. Predicting the probability of significant prostate cancer in Japanese men with serum prostate-specific antigen less than 10 ng/mL: development of a novel pre-biopsy nomogram. International Journal of Urology. 2010;17(3):274–280. doi: 10.1111/j.1442-2042.2010.02453.x. [DOI] [PubMed] [Google Scholar]
- 25.Yamamoto S. Editorial comment to predicting the probability significant prostate cancer in Japanese men with serum prostate-specific antigen less than 10 ng/mL: development of a novel pre-biopsy nomogram. International Journal of Urology. 2010;17(3):p. 280. doi: 10.1111/j.1442-2042.2010.02477.x. [DOI] [PubMed] [Google Scholar]
- 26.Kattan MW, Shariat SF, Andrews B, et al. The addition of interleukin-6 soluble receptor and transforming growth factor beta1 improves a preoperative nomogram for predicting biochemical progression in patients with clinically localized prostate cancer. Journal of Clinical Oncology. 2003;21(19):3573–3579. doi: 10.1200/JCO.2003.12.037. [DOI] [PubMed] [Google Scholar]